Fish hook open-globe injuries (OGIs) are challenging to repair surgically because of the backward-projecting barb near the hook’s point that prevents withdrawal of the hook. The most commonly reported ophthalmic surgical technique for removal of barbed hooks is advance-and-cut, wherein the fish hook is pushed through an iatrogenic wound to the exterior of the globe, the barb is cut off, and the shank is backed out of the entry wound. We report 2 cases of zone I OGIs with retained fish hooks successfully repaired using the back-out technique. This strategy involves enlarging the entry wound to allow the entire hook and barb to be backed out, decreasing iatrogenic injuries and eliminating the need for wire cutters.
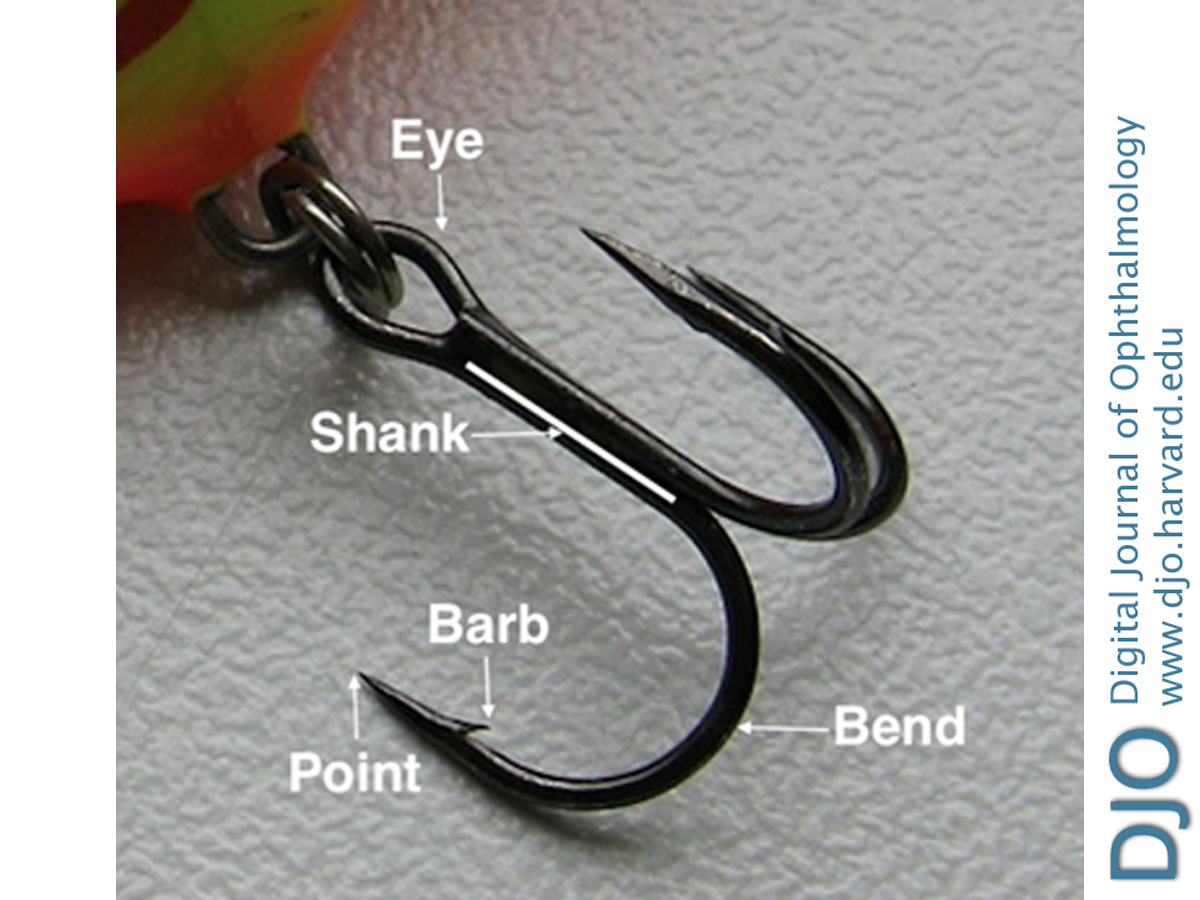
Open-globe injuries (OGIs) are an uncommon but debilitating form of injury, with the potential to cause significant ocular morbidity.(1) OGIs are estimated to affect 3.8 per 100,000 individuals in the United States annually.(2) One rare cause of OGI is fish hook–related trauma. Fish hook OGIs are challenging to repair surgically because of the pointed barb, designed to lodge in the flesh of the fish. This barb prevents easy removal of the hook from tissue through the entry wound and ensures that the hook can only travel forward, lodging itself deeper into impaled tissues (see Figure 1). The advance-and-cut method is the most commonly reported approach to remove intraocular barbed fish hooks. The technique involves pushing the hook through a surgical incision to the exterior of the globe, clipping the barb, and removing the shank of the hook backward through the entry wound.(3) Though effective, the technique has disadvantages, including the creation of an additional wound site, the requirement for wire cutters, and the potential for additional iatrogenic injury due to globe manipulation during wire cutting. Alternatively, the back-out method involves surgically enlarging the entry path of the barb in a controlled manner so it can be backed out of the tissue without damaging posterior structures during removal.(4-8) We describe 2 cases in which the back-out method was successfully used to remove fish hooks causing OGIs.
Case 1
A 20-year-old man presented to Massachusetts Eye and Ear from an outside hospital with a fish hook injury to the left eye. On examination, his visual acuity was counting fingers in the left eye. Intraocular pressure assessment was deferred, and pupillary assessment did not show a relative afferent pupillary defect (rAPD). The patient’s extraocular movements were full. His external examination was notable for a fish hook with attached organic material embedded in the central corneal stroma, with surrounding stromal edema; the hook had impaled a retained soft contact lens. The tip of the fish hook appeared to be in the anterior chamber. Seidel testing with provocation, performed with the patient’s contact lens still in place, was negative. Due to the risk of additional corneal damage or anterior chamber flattening, and the speed with which the patient was able to be brought to the operating room, the organic material was left in place while in the emergency department. His anterior segment examination revealed moderate conjunctival injection with ciliary flush, trace cells in a formed anterior chamber, and an intact iris and crystalline lens. Dilated fundus examination was normal. Computed tomography (CT) of the orbits revealed that the fish hook was in the anterior chamber, without a radiopaque intraocular foreign body in the vitreous cavity. Intravenous vancomycin and ceftazidime were initiated, and tetanus status was confirmed to be up to date.
Removal of the foreign body and repair of presumed zone I OGI was performed under general anesthesia (Video 1). First, the contact lens was carefully removed. Intraoperatively, with better visualization of the anterior segment, a full-thickness corneal wound in the temporal peripheral cornea was noted. This injury was consistent with an exit wound, where the fish hook must have penetrated the cornea and subsequently retracted, with the barb embedding in the stroma near the entrance site, with the tip of the fish hook still in the anterior chamber.
A paracentesis was made at 10 o’clock, and the anterior chamber was inflated with sodium hyaluronate. Using a 15° blade, a partial thickness cut was made in the anterior stroma overlying the fish hook, in the same axis as the barb, traversing the entire length of the embedded hook. Using a cyclodialysis spatula to evert the edges of the partial-thickness cut, the hook was backed out carefully from the cornea and removed. At this time, a full-thickness stellate wound was seen at the hook entry point and closed using two 10-0 nylon sutures in an “X” configuration. A single 10-0 nylon suture closed the exit wound temporally, and fluorescein dye confirmed a watertight seal.
Given the exposure to organic matter and aquatic pathogens, intrastromal moxifloxacin and amphotericin were administered to the corneal stroma around the wounds; intracameral moxifloxacin was injected into the anterior chamber. A subconjunctival steroid and antibiotic injection was administered away from the laceration.
Postoperatively, the patient was admitted for 48 hours of intravenous antibiotics. At his most recent follow-up appointment (1 month after injury), his pinhole visual acuity was 20/70, and his anterior chamber formed. His anterior segment examination revealed resolving central corneal microcystic edema and Descemet membrane folds around the wounds and along the trajectory of the hook. His crystalline lens remained clear, and dilated fundus examination was unremarkable.
Case 2
A 59-year-old man presented at Massachusetts Eye and Ear from an outside hospital with a fish hook injury to the left eye. He was fly casting when the wind blew the hook backward, causing the barbed hook to impale the eye.
On presentation, the patient’s visual acuity was 20/600, pinholing to 20/200. Intraocular pressure assessment was deferred, and pupillary assessment did not reveal an rAPD. The patient’s extraocular movements were full. On gross examination, the patient had a barbed, single-pronged fish hook in the left eye embedded into the central cornea (Figure 2A). Slit-lamp examination revealed corneal stromal edema surrounding the hook. The anterior chamber had a hazy view, with 1+ cells and no hypopyon or hyphema. The iris and lens appeared intact. It could not be determined whether the tip of the hook was still embedded in the posterior corneal stroma or whether it had penetrated the corneal endothelium into the anterior chamber. Dilated fundus examination was normal. CT of the orbits revealed that the fish hook was embedded in the anterior globe, without a radiopaque intraocular foreign body in the vitreous cavity. Intravenous vancomycin and ceftazidime were initiated, and a recent tetanus booster was confirmed.
Removal of the foreign body and repair of the zone I OGI was performed under general anesthesia. On initial review, the barb was embedded in the mid-stroma, with no obvious exit wound. The fish hook shank was grasped with a large needle-driver but could not be removed because of the barb. Using a 15° blade, the corneal stroma overlying the fish hook was cut along the same axis as the barb in a partial-thickness manner traversing the entire length of the embedded hook. The edges of the stromal cut were everted, and the hook was carefully backed out and removed from the cornea, subsequently demonstrating that there was a full-thickness defect in the cornea. A paracentesis was made temporally, and sodium hyaluronate was injected to reform the anterior chamber. The 1.5 mm laceration across the central cornea was closed with two interrupted 10-0 nylon sutures. The sodium hyaluronate was thoroughly irrigated with balanced salt solution through the paracentesis. Intracameral moxifloxacin was injected, and subconjunctival steroid and antibiotic injection was performed away from the laceration. The patient was then admitted for a 2-day course of systemic vancomycin and ceftazidime.
Postoperatively, the patient’s visual acuity improved steadily. At his most recent follow-up, 5 months after his injury, visual acuity was 20/30, pinholing to 20/25-2, intraocular pressure was 15 mm Hg, and extraocular movements were full. Slit-lamp examination demonstrated a paracentral corneal stromal scar with adjacent small stromal scars in the prior nylon suture tracks (Figure 2B). The iris was slightly oblong and had a transillumination defect at the 5:00 position. The lens was notable for mild nuclear sclerosis and a small area of anterior capsular fibrosis with pigment superiorly. Fundus examination was unremarkable.
Video 1.
Overview of the key surgical points during the extraction of an intraocular fish hook for case 1. Briefly, a partial thickness cut was made into the anterior stroma overlying the fish hook, which was then backed out carefully from the cornea and removed. A single 10-0 nylon suture closed the exit wound temporally, and fluorescein dye confirmed a watertight seal.
Figure 2.
Case 2. A, On presentation, gross examination was notable for a single-pronged fish hook with organic material embedded in the central cornea. B, Gross examination at 5 months postoperatively revealed a well-healed paracentral corneal scar with adjacent small stromal scars from the prior nylon sutures.
Open-globe injuries involve full-thickness trauma to the cornea and/or sclera and have the potential for severe vision loss. Demographically, they tend to occur in males, are often due to work-related injuries, and have a reported incidence around 3.8 per 100,000.(2) They are categorized by mechanism and zone of injury. The 2 cases reported here were zone I injuries with fish hook intraocular foreign bodies, the first involving a perforating open globe injury (ie, with both an entrance and exit wound) and the second involving a penetrating open globe injury (ie, with entrance wound alone).
Fish hook injury is a rare but potentially devastating ocular insult. The hooks can be deeply embedded, and the barb prevents backward retreat, thus posing a surgical challenge. The body of literature on this unique presentation is growing, and four approaches for fish hook removal have been described. The “snatch” technique entails looping string around the hook bend nearest the skin, pressing the eye of the hook down then out as if to back the hook out, and quickly yanking backward on the string in a parallel plane to the skin; it is not recommended for ocular fish hook injuries. The advance-and-cut method involves pushing the point of the hook through to the outside of the eye, where the point and barb can be cut off. The shank, which is often too large to be pushed all the way through, is then backed out via the entry wound. For fish hook injuries involving the retina, the needle-cover method involves inserting a needle into the entry wound, securing the barb with the lumen of the needle, and backing both out together. Finally, the back-out method entails moving the hook backward along its path of entry; this method is generally reserved for barbless hooks.
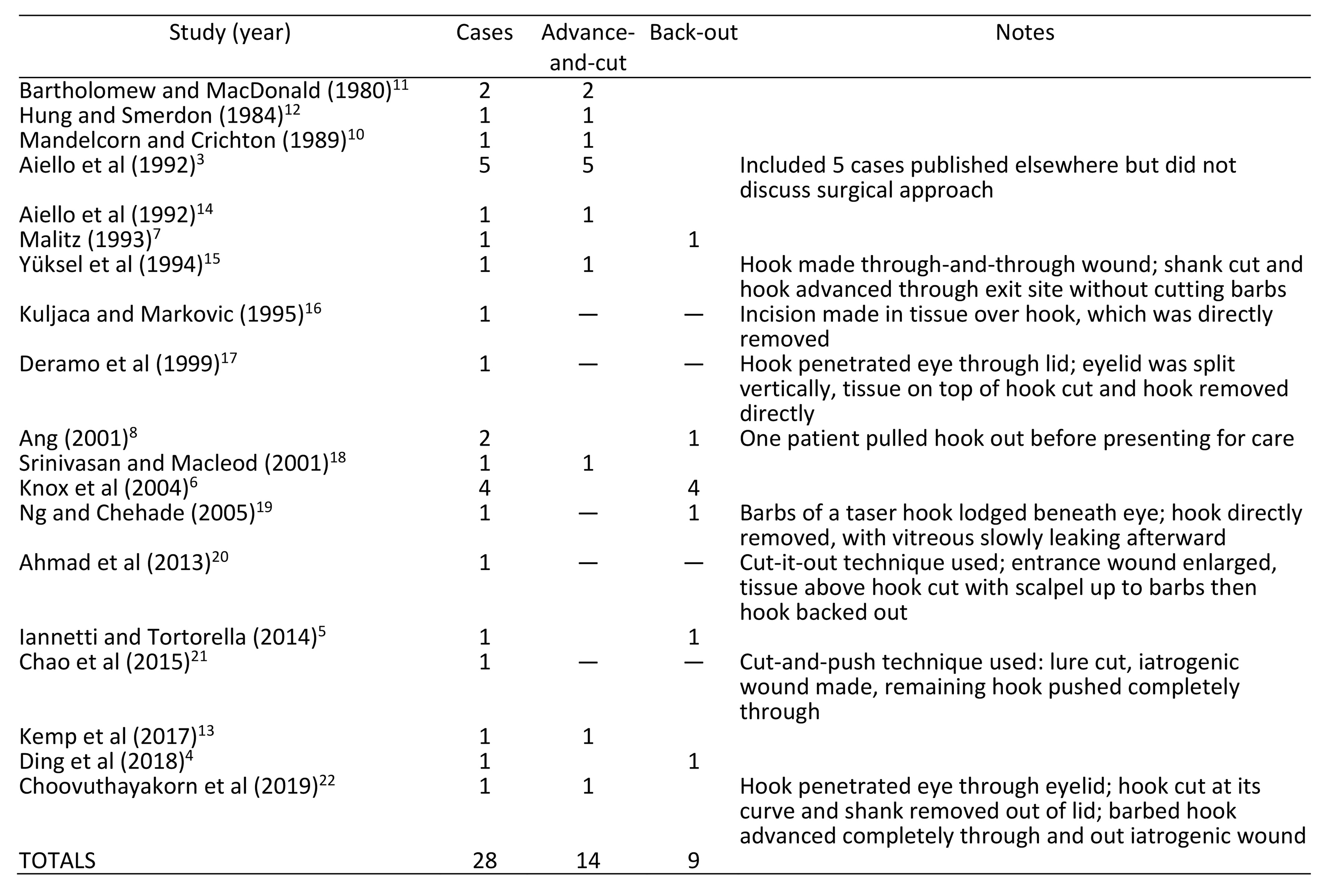
Although success has been reported using the back-out method for barbless fish hook injuries,(9) the advance-and-cut technique has been touted as the ideal approach for barbed hooks,(3) with multiple cases of excellent outcomes reported.(10-13) Indeed, an in-depth review of the literature returned 19 publications (28 patients) addressing surgical approach for intraocular fish hooks: 14 involving the advance-and-cut method, 9 the back-out method, and the rest a mix of other approaches (Table 1). It is notable that when an ophthalmologist is dealing with central corneal wounds, the advance-and-cut method for removing a barbed fish hook through the peripheral corneal stroma allows for repair of a less astigmatic-inducing wound and minimization of additional iatrogenic central corneal trauma. Suturing of a larger central corneal wound can flatten the central cornea and result in additional refractive error. In our cases, the back-out method was used by first enlarging the entry site to create a track for the barb to minimize additional sites of iatrogenic trauma. Malitz was the first to publish use of this technique successfully in an ocular setting with a barbed hook in 1993, and several other cases have been reported with similarly positive outcomes.(3-7) The vision results in our cases provide further evidence of the technique’s utility in removing barbed hooks.
The advance-and-cut method has several disadvantages relative to the back-out method. First, fish hooks, being a tool for holding bait (eg, worms), are often contaminated with multiple pathogens; using such a device to create an iatrogenic wound might theoretically increase the risk of infection. Additionally, ophthalmologists rarely have access to, or experience using, wire cutters in the operating room as required for the advance-and-cut method. This is even more true in resource-limited settings or in ambulatory surgery centers. In the process of transecting the barb from the hook, the pressure exerted by the wire cutters on the fish hook may also cause unintended rotation and movement of the hook, producing additional iatrogenic damage in the process. Knox et al pointed out that the advance-and-cut method is not as suitable for small hooks, because they require significant manipulation to push through compared to a hook with a large-diameter bend.(6) In the cases presented here, the tip of the hook and barb had come to rest in the corneal stroma, and the back-out method enabled facile removal.
In addition to the back-out surgical technique, we administered intraocular and systemic antibiotics and undertook surgical repair within 24 hours of injury, which may be critical to ensuring good visual acuity outcomes.(3,7,23) We instilled intracameral moxifloxacin in case 1, in addition to hydrating the corneal stroma of the wound edges with amphotericin and moxifloxacin, as described previously for management of recalcitrant microbial keratitis and adopted here for prophylaxis.(24) In case 2, intracameral moxifloxacin was also administered, but injections in the wound edges were not performed. These prophylactic measures, in addition to prompt globe repair with the use of the back-out technique to remove the hook, may have contributed to the uncomplicated course and good visual outcomes to date.
Both of our patients had an uncomplicated postoperative course with marked improvement in visual acuity. These results add to the body of literature demonstrating the effectiveness of the less frequently employed back-out method for treating barbed fish hook OGIs. A comparison of cases repaired with the advance-and-cut versus back-out methods is warranted to identify potential differences in complication rates or indications for one surgical technique over the other.
Literature Search
PubMed was searched on June 25, 2020, resulting in 31 relevant and accessible publications. The references section of each paper was reviewed for additional papers, yielding a total of 38 publications. Publications on fish hook trauma to the eyelid without globe involvement were not included in Table 1; nor were cases that did not involve a barbed hook. The following terms were searched: ocular fish hook, open globe AND fish hook, ruptured globe AND fish hook, case report AND eye fish hook, case report AND open globe fish hook, eye surgery AND fish hook, penetrating ocular AND fish hook, ocular AND fishhook.
Acknowledgments
Alexander Pomerantz has equity in Johnson & Johnson, Pfizer, Eli Lilly, and Medtronic; Grayson Armstrong, MD, is a cofounder of an ophthalmic telemedicine company Ocular Technologies, an advisor to Kriya Therapeutics, and an advisor for Eko Technologies.
1. Rahman I, Maino A, Devadason D, Leatherbarrow B. Open globe injuries: factors predictive of poor outcome. Eye 2006;20:1336-41.
2. Ramirez DA, Porco TC, Lietman TM, Keenan JD. Ocular injury in United States emergency departments: seasonality and annual trends estimated from a nationally representative dataset. Am J Ophthalmol 2018;191:149-55.
3. Aiello LP, Iwamoto M, Guyer DR. Penetrating ocular fish-hook injuries: surgical management and long-term visual outcome. Ophthalmology 1992;9:862-6.
4. Ding X, Liu Z, Lin Y, Yang Y. Perforating ocular fishhook trauma: a case report. Clin Exp Optom 2018;101:297-8.
5. Iannetti L, Tortorella P. Penetrating fish-hook ocular injury: management of an unusual intraocular foreign body. Case Rep Med 2014;2014:901285.
6. Knox FA, Chan WC, McAvoy CE, Johnston SE, Bryars JH. Penetrating ocular injuries from fish-hooks. International Ophthalmology 2004;25:291-4.
7. Malitz DI. Fish-hook injuries. Ophthalmology 1993;100:3.
8. Ang CS. Ocular fishhook injuries. Med J Malaysia 2001;56:252-4.
9. Agrawal R, Laude A, Taneja M. Fish-hook injury of the eye. Int Ophthalmol [Internet]. 2012;32:269-71. http://www.ncbi.nlm.nih.gov/pubmed/22456795.
10. Mandelcorn MS, Crichton A. Fish hook removal from vitreous and retina. Arch Ophthalmol 1989;107:493.
11. Bartholomew R, MacDonald M. Fish hook injuries of the eye. Br J Ophthalmol 1980;64:531-3.
12. Hung SO, Smerdon D. Eyeball injury due to fish hook. J Trauma 1984;24:997-8.
13. Kemp PS, Shah AS, Elliott AT, Wan MJ. Removal of a barbed fish hook from the cornea of an 8-year-old boy. J AAPOS 2017;21:407.e1.
14. Stryjewski TP, Andreoli CM, Eliott D. Retinal detachment after open globe injury. Ophthalmology 2014;121:327-33.
15. Liang SYW, Lee GA. Intrastromal injection of antibiotic agent in the management of recalcitrant bacterial keratitis. J Cataract Refract Surg 2011;37:960-2.
16. Aiello LP, Iwamoto M, Taylor HR. Perforating ocular fishhook injury. Arch Ophthalmol 1992;110:1316-7.
17. Yüksel N, Elibol O, Ca?lar Y. Penetrating corneal fish-hook injury. Ophthalmologica 1994;208:112-3.
18. Kuljaca Z, Markovic P. Penetrating ocular fish-hook injury. Eye (Lond) 1995;9 (Pt 3):385-6.
19. Deramo VA, Maus M, Cohen E, Jeffers J. Removal of a fishhook in the eyelid and cornea using a vertical eyelid-splitting technique. Arch Ophthalmol 1999;117:541-2.
20. Srinivasan S, Macleod S. Fish hook injury to the eyelid—an unusual case. Indian J Ophthalmol 2001;49:115-6.
21. Ng W, Chehade M. Taser penetrating ocular injury. Am J Ophthalmol 2005;139:713-5.
22. Ahmad SS, Seng CW, Ghani SA, Lee JF. Cut-it-out technique for ocular fish-hook injury. J Emerg Trauma Shock 2013;6:293-5.
23. Chao DL, Erickson BP, Rachitskaya AV. Penetrating ocular fishhook injury. JAMA Ophthalmol 2015;133:347-8.
24. Choovuthayakorn J, Chavengsaksongkram P, Watanachai N, Chaidaroon W. Penetrating eyelid and ocular fishhook-related injury. Case Rep. Ophthalmol 2019;10:41-6.
 Welcome, please sign in
Welcome, please sign in