|
|
 |
|
|
|
|
|
Floating anterior lens capsule: an unusual case of true exfoliation
Digital Journal of Ophthalmology
2010
Volume 16, Number 4
November 29, 2010
DOI: 10.5693/djo.02.2010.10.001
|
Printer Friendly
Download PDF |
|
|
|
|
|
|
| Abstract | Summary
A rare case of delamination and replication of the anterior lens capsule into prominent floating folds in the anterior chamber approximately 55 years after a penetrating injury to the eye and anterior lens capsule is reported. Classically, true exfoliation of the anterior lens capsule has been reported in individuals who have been exposed to intense heat over a prolonged period. However, more recently cases of true exfoliation of the anterior lens capsule have been reported in patients who have not been occupationally exposed to high temperatures and associated infrared radiation. A brief review of the literature concerning true exfoliation of the lens capsule in the absence of intense heat exposure is included. Associations with trauma, inflammation, advanced age, hyperopia, glaucoma, and capsular protein abnormality have been reported, but the pathogenesis of this rare clinical finding remains conjectural. | | | Case Report | An 88-year-old, white man presented with a complaint of gradually decreasing vision over many months. He related a history of sustaining an injury to his left eye in 1944 while serving in the Army in France during World War II. On questioning, the patient denied an occupational exposure to the intense heat.
Uncorrected visual acuity was recorded as 20/70 in the right eye and 20/80-2 in the left eye. Following manifest refraction visual acuity was 20/40 in the right eye and 20/80 in the left eye. The salient features of the examination pertained to the anterior segments. Slit-lamp examination of the cornea and anterior chamber of the right eye was normal. Examination of the left cornea disclosed an approximately 3 to 4 mm, full-thickness stromal scar in an oblique orientation at the superior limbal area (Figure 1). Careful slit-lamp examination of the anterior chamber in this eye revealed a diaphanous membrane in a multiple fold pattern that undulated slowly on eye movement and exhibited a petaloid appearance.
It was apparent that this membranous structure emanated from within the pupil and was not adherent to the iris or cornea at any point. Dilated examination revealed a moderately dense, brunescent, nuclear cataract in the right eye and a very dense, brunescent, nuclear cataract in the left eye. There was also noted to be a small anterior subcapsular cataract centrally in the left eye. When the pupil was dilated, the membrane assumed a relatively unfolded pattern (Figures 2 and 3).
On examination, the folds could be seen to originate from the area of the anterior subcapsular lens opacity. Gonioscopic examination was normal bilaterally without suggestion of pseudoexfoliation material in the angle. Funduscopic examination revealed only mild retinal pigment epithelial alteration in the macular regions and reticular pigmentary degeneration of the peripheral retina bilaterally.
The patient was offered cataract surgery for the left eye on multiple occasions but declined to undergo the procedure. | |

Figure 1
Left eye showing corneal stromal scar (arrow).
|
|
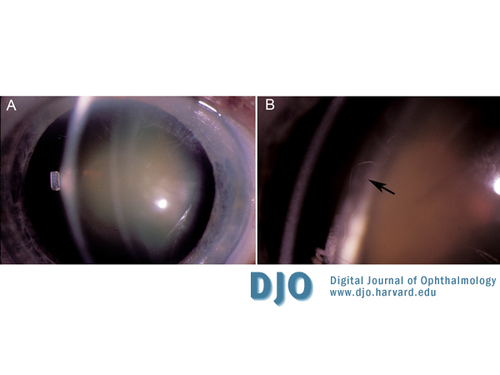
Figure 2
Low- (A) and high-power (B) photographs of patient’s left eye with dilated pupil showing floating anterior lens capsule (arrow points to edge of floating anterior capsular fold).
|
|
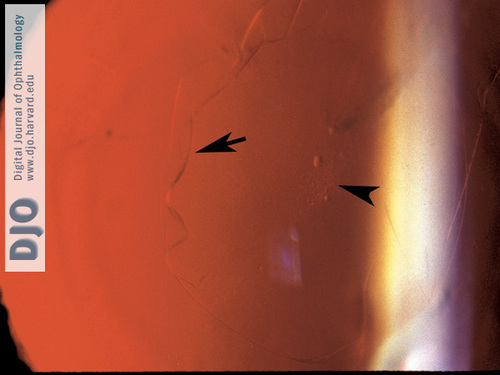
Figure 3
Left eye showing edge of floating anterior capsular fold on retro-illumination (arrow) and anterior subcapsular cataract opacity (arrowhead).
|
|
| Discussion | Information concerning floating folds of the anterior lens capsule is very sparse. Duke-Elder mentions the subject only briefly and described it as an exceptional occurrence.(1) He referenced a unique case reported by Punder in 1956 that was associated with a complicated cataract.(2) On histological examination, fan-shaped folded extensions of the anterior capsule were found floating freely in the anterior chamber. Interestingly, the photomicrograph from this case revealed the underlying lens epithelium to be in association with the capsular folds. This finding has not been noted elsewhere.
Burde et al. published the first electron microscopic study of true exfoliation of the lens capsule in a 77-year-old white man in 1969.(3) The individual had sustained a blunt injury to the left eye in 1944 and several years later developed a cataract. He had also been employed for 20 years as a foundry worker in a steel mill, where he worked in front of a furnace without the benefit of protective goggles. On slit-lamp examination, there was noted to be a fine gossamer membrane attached to the anterior surface of the lens with a free edge floating in the anterior chamber. Following intracapsular cataract surgery, the specimen was examined by electron microscopy. In the involved area, there was noted to be a split of the fibrillar laminated sheets in the outer one-third of the capsule. The underlying epithelial cells were described as appearing normal. The location of the rent in the lens capsule was correlated with the area clinically noted to be the origin of the fine gossamer membrane. Additional electron microscopic studies of cases of true exfoliation of the anterior lens capsule have demonstrated similar findings.(4-6) In some instances, the underlying epithelial cells have been reported as abnormal. This anterior capsular delamination and true exfoliation has also been demonstrated by ultrasound biomicroscopy.(7)
In 1954 Theobold initially differentatiated between the two pathologic entites of true and pseudoexfoliation of the lens capsule.(8) She described the clinical picture of true exfoliation of the lens capsule as that of a glasslike membrane peeling off the lens capsule in the pupillary zone. These cases were in individuals with occupational exposure to intense heat and associated infrared radiation.
Some cases in the literature note material similar to that initially described by Theobold deposited in the pupillary area without patient history of exposure to high heat. Trauma and inflammation are purported to be inciting factors in the development of true exfoliation of the lens capsule in these cases.(9) Cashwell et al reported a series of 11 such eyes in 7 patients who had not had exposure to intense heat or ocular trauma.(10) Interestingly, 5 of these 7 patients had been diagnosed with glaucoma. All of these patients had reached an advanced age (average, 85 years). It is further noteworthy that the refractive error in all these 7 patients was hyperopic and varied from a spherical equivalent of +1.00 D to + 7.25 D. A possible relationship between the anatomy of the hyperopic lens and the occurrence of true exfoliation of the lens capsule thus has been suggested. Also, abnormalities in protein components of exfoliated lens capsule have been demonstrated following analysis.(4)
It is quite likely that there may be some as yet unknown common pathogenic mechanism regarding the development of true exfoliation of the lens capsule secondary to intense heat and the delamination of the anterior lens capsule in cases without infrared radiation exposure. A review of the literature suggests that there may be a relationship not only to trauma but also to glaucoma, hyperopia, and abnormalities of protein components of the lens capsule. However, the basic pathologic process resulting in the delamination and subsequent replication of the lens capsule into the prominent floating folds exhibited in this case has not been established. In the patient presented here, the intraocular pressures were recorded in the low teens, and his optic nerve heads were well vascularized, without suggestion of glaucomatous cupping. In addition, his manifest refractive error was +3.25 D sphere in each eye. Given these data, it seems likely that his exfoliation of the anterior lens capsule occurred secondary to trauma approximately 55 years ago. | | | References | 1. Duke-Elder S. System of Ophthalmology. Volume 11, Diseases of the Lens and Vitreous, Glaucoma and Hypotony. St. Louis, MO: CV Mosby; 1969:57-58.
2. Pünder H. Fluctuating capsular folds, a rare lenticular finding in complicated
cataract. Klin Monatsbl Augenheilkd 1956;129:98-101.
3. Burke RM, Bresnick G, Uhrhammer J. True exfoliation of the lens capsule. Arch Ophthalmol 1969;82:651-3.
4. Anderson IL, Van Bockxmeer FM. True exfoliation of the lens capsule: a clinicopathologic report. Aust NZ J Ophthalmol 1985;13:343-7.
5. Karp CL, Fazio JR, Culbertson WW, Green WR. True exfoliation of the lens capsule. Archives of Ophthalmol 1999;117:1078-80.
6. Majima K, Kousaka M, Kanbara Y. A Case of true exfoliation. Int J Ophthalmol 1996;210:341-3.
7. Hwang YS, Chang SH. Ultrasound biomicroscopy of capsular delamination (true exfoliation) of the crystalline lens. Chang Gung Med J 2003;26: 930-2.
8. Theobold GD. Pseudoexfoliation of lens capsule: Relations to “true” exfoliation of lens capsule as reported in the literature and role in production of glaucoma capsulare. Am J Ophthalmol 1954;37:1-12.
9. Brodrick JD, Tate GW. Capsular delamination (true exfoliation) of the lens: report of a case. Arch Ophthalmol 1979;97:1693-8.
10. Cashwell LF, Holleman IL, Weaver RG, van Rens GH. Idiopathic true exfoliation of the lens capsule. Ophthalmology 1989;96:348-51. | |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in 




