|
|
 |
|
|
|
|
|
The best of the best: a review of select glaucoma case reports published in 2015
Digital Journal of Ophthalmology 2016
Volume 22, Number 4
December 31, 2016
DOI: 10.5693/djo.01.2016.06.001
|
Printer Friendly
Download PDF |
|
|
 Ambika Hoguet, MD
Ambika Hoguet, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School Louis R. Pasquale, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School Channing Division of Network Medicine, Brigham and Women’s Hospital
|
|
|
| Abstract | | This review article summarizes four key case reports published in the field of glaucoma in the year 2015. The first article describes a novel technique for draining choroidal fluid in patients with uveal effusion syndrome. The second article describes 2 cases of recurrent vitreous block despite adequate surgical intervention. The third article describes 2 cases of endogenous steroid response glaucoma. The last article describes the treatment of visual phenomena following iridectomy using femtosecond laser assisted keratopigmentation. | | | Body | Introduction
In 2014 we reviewed 4 of the 84 case reports that were published in the field of glaucoma (as indexed in MEDLINE). As our understanding of the clinical and surgical management of glaucoma continues to evolve, reviewing case reports remains an indispensable way to advance our knowledge in the field. A well-written case report can provide information about the unique presentation of disease, novel therapeutic approaches, innovative surgical techniques, and uncommon but important outcomes of medical and surgical interventions.
As a reflection of our growing fund of knowledge, in the year 2015, 126 case reports in the field of glaucoma were published in English (as indexed in MEDLINE). To assess which articles have the greatest potential for impacting current practice, we graded each publication with respect to the following parameters: (1) potential to improve patient care, (2) unique clinical case or management technique, (3) comprehensive description of the clinical or surgical scenario, and (4) use of appropriate images when indicated. Here we summarize what we consider to be the most clinically relevant publications of the year.
Ex-PRESS shunt for choroidal fluid drainage in uveal effusion syndrome type 2
In this retrospective case series, Yepez and Arevalo present 3 eyes of 2 patients with uveal effusion syndrome without coexisting nanophthalmos (type 2) who underwent implantation of an Ex-PRESS shunt (Alcon Laboratories).(1) Uveal effusion syndrome is a rare, relapsing-remitting disease characterized by uveal effusion with ciliochoroidal detachment in patients with a thick and impermeable sclera. Presenting signs include dilated episcleral vessels, thickened or detached choroid and ciliary body, and nonrhegmatogenous retinal detachment.(2) The traditional treatment involves a full-thickness sclerotomy or sclerostomy especially in eyes that are smaller than average size (<23 mm), or vortex vein decompression.(3) However, vortex vein decompression can be challenging, and response to treatment with either of these approaches is variable with common recurrences (23%-50%).(1)
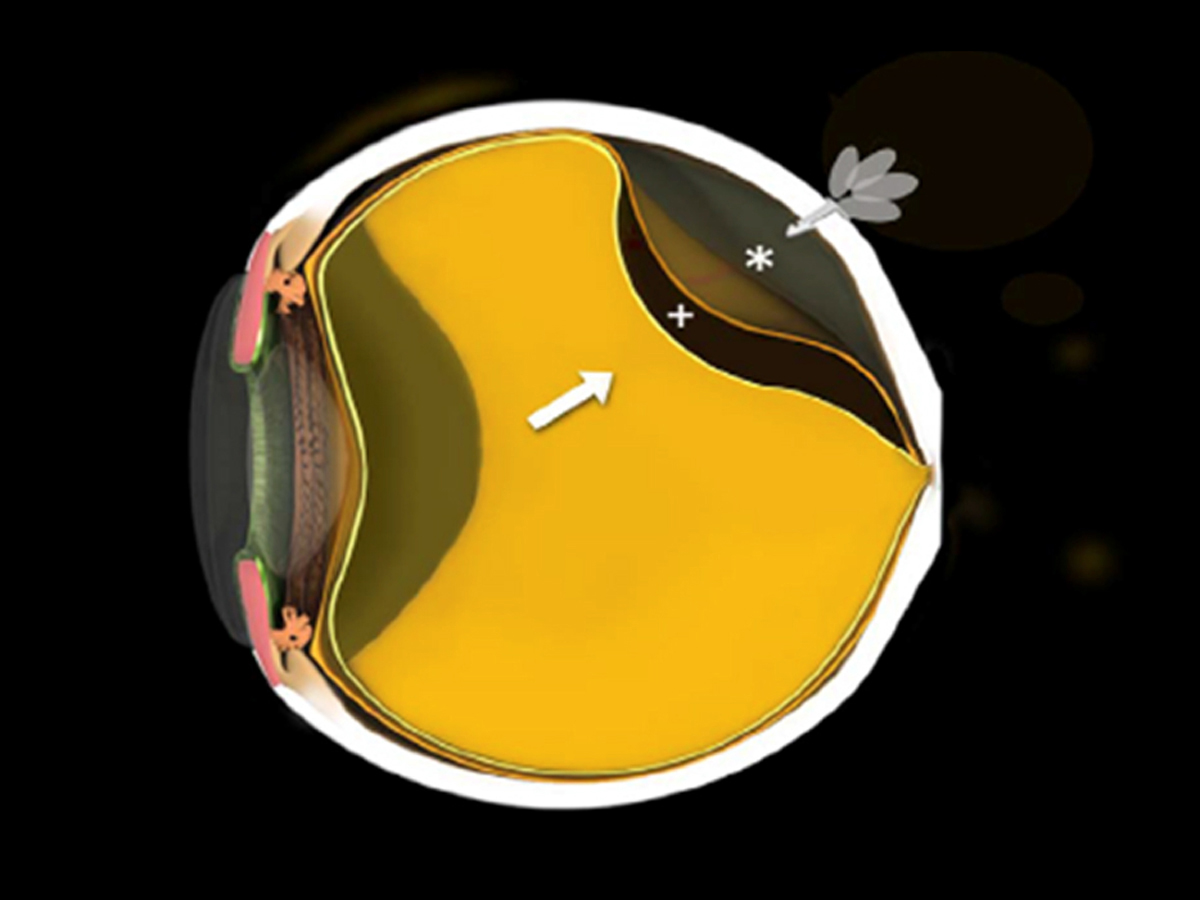
In the 3 eyes in this series, the ex-PRESS shunt (model P-50) was inserted into an oblique sclerotomy 13 mm posterior to the limbus to allow drainage of suprachoroidal fluid (Figure 1). All eyes showed improvement in visual acuity (presenting vision of 20/200 to 20/400) to 20/30 or better and maintained this visual acuity through 24 months’ follow-up.
The Ex-PRESS shunt may facilitate a constant drainage from the suprachoroidal space to the subconjunctival space, thereby lowering the recurrence rate of uveal effusion in these patients. More studies are needed to determine whether this technique is useful in patients with recurrent disease.
Recurrence of aqueous misdirection following pars plana vitrectomy in pseudophakic eyes
Vitreous block, also referred to as aqueous misdirection or malignant glaucoma, describes a type of secondary angle closure glaucoma where abnormal fluid movement through the vitreous leads to anterior rotation of the ciliary body. Clinical features include a uniformly shallow anterior chamber despite a patent iridectomy and elevated intraocular pressure (IOP). It is a rare condition that usually occurs following intraocular laser or incisional surgery, but can occur without surgery as well.(4) Treatment is aimed at reestablishing the flow of aqueous from the vitreous to the anterior chamber. Medical therapy includes cycloplegia and hyperosmotics, but this often results in a high rate of recurrence.(5) Laser treatment involves a posterior capsulotomy if the patient is pseudophakic; however, this can result in a high rate of recurrence as well, up to 30% in 3 months.(6) Surgical intervention with a pars plana vitrectomy, anterior hyaloidotomy, and iridectomy is most successful in preventing recurrences.(5)
In this retrospective, interventional case series, Dave et al present 4 patients who developed recurrent aqueous misdirection following pars plana vitrectomy, zonulectomy, and iridectomy for malignant glaucoma.(7) An obstruction of aqueous flow through the communication created following surgical treatment was present in all patients (Figure 2). This occurred because of an inflammatory membrane covering the hyaloidotomy opening in 3 eyes and the haptic of the lens blocking the hyaloidotomy opening in 1 eye. In the last-named case, a Nd:YAG hyloidotomy resolved the problem. In the cases where the iridectomy was obstructed, laser membranotomy restored the aqueous flow. All cases had a successful outcome following laser treatment, up to 24 months’ follow-up.
In cases of recurrent vitreous block, it is important to look for signs of impeded aqueous flow. Recurrence can occur not only because of persistence of the anterior hyaloid but also because of postoperative changes that result in blockage of aqueous from the posterior to the anterior chamber.
Functional pituitary tumors masquerading as primary glaucoma and effect of hypophysectomy on intraocular tension
The use of corticosteroids can lead to a high IOP and an increased risk of glaucoma in 18%-36% of patients.(8) Of patients with steroid-induced glaucoma, 26.5% eventually require trabeculectomy for optimum IOP control.(9) In this case series, Gupta et al present 2 patients with endogenous, steroid-induced ocular hypertension.(9) In the first case, the patient presented with physical signs of hypercortisolism, including truncal obesity, pedal edema, and hirsutism in addition to elevated IOP. The patient was diagnosed with adrenocorticotropic hormone-dependent Cushing syndrome, and the IOP normalized following a transsphenoidal hypophysectomy. In the second case, the patient had bilateral iridectomies for narrow angles and borderline intraocular pressures that were initially well controlled on topical latanoprost. However, 1.5 years later, the patient developed elevated IOP despite maximal medical therapy. On further evaluation, large hands and feet and gynecomastia were noted. Further workup revealed presence of a hormone-secreting pituitary adenoma, and his IOP was controlled after resection of the adenoma. One year later, recurrence of the tumor was diagnosed with another IOP increase.
In conditions where previously well controlled IOP subsequently becomes elevated despite maximal medical therapy, it is important to look for additional risk factors. In both these cases a thorough review of systems and systemic examination revealed features of hormonal imbalance. Treatment of the underlying condition led to IOP control.
Femtosecond laser-assisted keratopigmentation for the management of visual disabilities due to peripheral iridectomies
Iris defects from iridectomies cause visual aberrations like shadows, ghost images, crescents, or lines in a small percentage of patients.(10) In patients with these symptoms, keratopigmentation on the cornea directly in front of the iridectomy can make the light that passes through the iridectomy more diffuse, blurring the image cast on the retina and eliminating any perceived visual aberrations.
In this report, Ricardo et al describe 2 patients who underwent femtosecond laser–assisted keratopigmentation for moderate-to-severe dysfunction secondary to peripheral iridectomies.(11) Cosmetic contact lenses were tried previously without success in both patients. The AMO 60KHz IntraLase femtosecond laser was used to create a stromal pocket of the desired dimension for pigmentation, and black and brown, alcohol-based, steam-sterilized tattoo pigments were then injected through the entry cut (Figure 3). This method allowed more precise, less invasive keratopigmentation in comparison to previously described techniques, such as intralamellar staining and superficial corneal staining. In both cases, visual symptoms of ghosting, glare, and monocular diplopia improved greatly.
Although not common, visual symptoms that result from a peripheral iridectomy can be extremely bothersome to patients. Femtosecond laser-assisted keratopigmentation offers a minimally invasive treatment to alleviate these visual phenomena. | |

Figure 1
Diagram reproduced from Yepez and Arevalo demonstrating insertion of the Ex-PRESS shunt into the sclerotomy, allowing drainage of suprachoroidal fluid.(1) Reprinted with permission, JAMA Ophthalmology.
|
|

Figure 2
A slit-lamp photograph reproduced from Dave et al showing an inflammatory membrane blocking the hyaloidectomy.(7) This disrupted communication of aqueous from the posterior to the anterior chamber, resulting in a recurrence of vitreous block. Reproduced with permission, British Medical Journal.
|
|

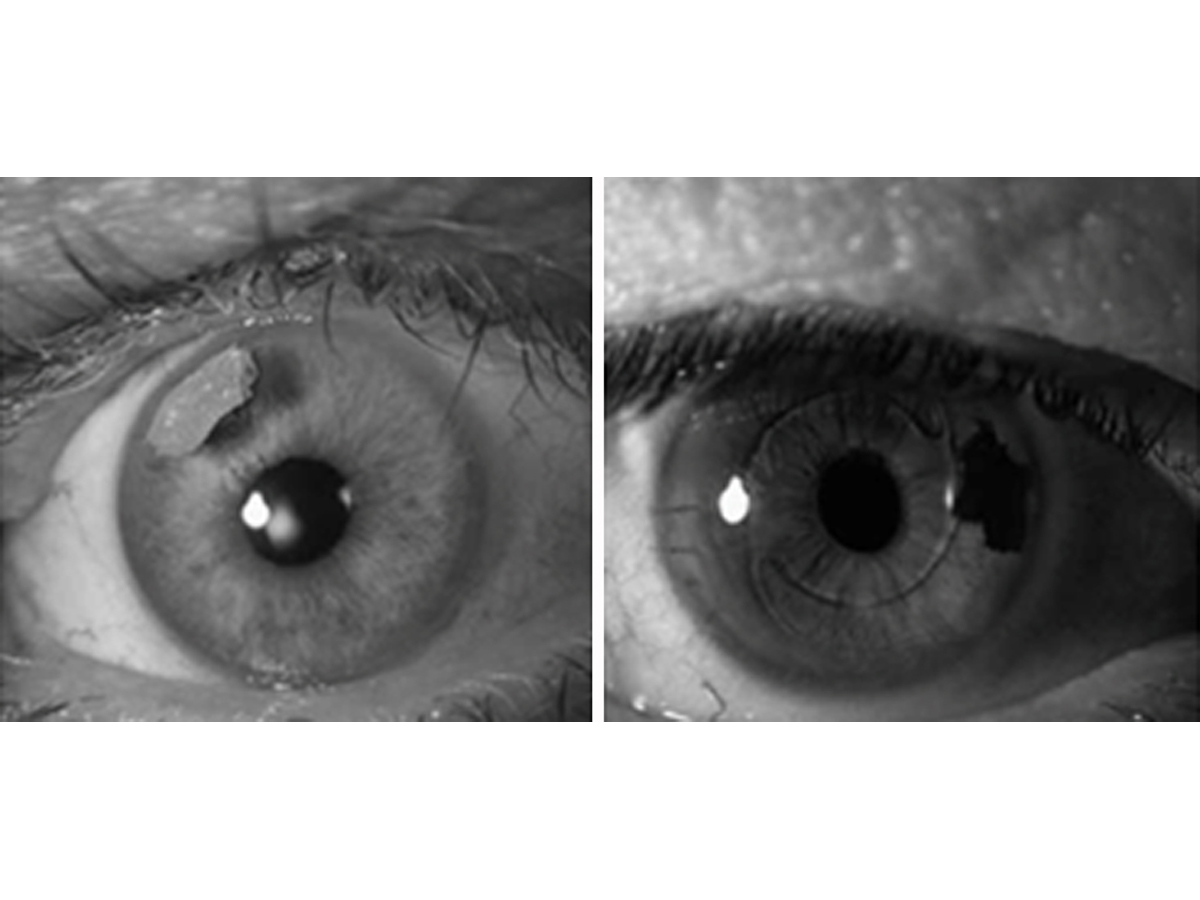
Figure 3
Appearance of eyes treated with femtosecond laser-assisted keratopigmentation over a superior and a temporal iridotomy. In both patients, visual symptoms of glare, ghosting, and monocular diplopia improved after treatment. Photographs courtesy of Dr. Roberto Pineda, MD.
|
|
| Summary | • Using an Ex-PRESS shunt may minimize the rate of recurrences of choroidal effusion in patients with uveal effusion syndrome.
• Recurrent vitreous block can occur because of postoperative changes that block the communication of aqueous from the posterior to the anterior chamber.
• A thorough review of systems and systemic examination is important in patients presenting with elevated intraocular pressures that are unresponsive to topical therapy.
• Femtosecond laser-assisted keratopigmentation is useful technique for alleviating visual aberrations in patients with laser peripheral iridectomies.
| | | References | 1. Yepez JB, Arevalo F. Ex-PRESS shunt for choroidal fluid drainage in uveal effusion syndrome type 2: a potentially novel technique. JAMA Ophthalmology 2015:133;470-71.
2. Uyama M, Takahashi K, Kozaki J, et al. Uveal effusion syndrome: clinical features, surgical treatment, histologic examination of the sclera, and pathophysiology. Ophthalmology 2000;107:441-9.
3. Damjji KF, Freedman S, Moroi S, et al. Shields Textbook of Glaucoma. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.
4. Kaplowitz K, Yung E, Flynn R, Tsai JC. Current concepts in the treatment of vitrous block, also known as aqueous misdirection. Surv Ophthalmol 2015; 229-241
5. Debrouwere V, Stalmans,P, Van Calster J, et al. Outcomes of different management options for malignant glaucoma: a retrospective study. Graefes Arch Clin Exp Ophthalmol 2012; 250:131-41.
6. Dave P, Senthil S, Rao HL, Garudadri CS. Treatment outcomes in malignant glaucoma. Ophthalmology 2013;120:984-90.
7. Dave P, Rao A, Senthil S, Choudhari NS. Recurrence of aqueous misdirection following pars plana vitrectomy in pseudophakic eyes. BMJ Case Rep. doi: 10.1136/bcr-2014-207961.
8. Tripathy RC, Parapuram SK, Tripathy BJ, Zhong Y, Chalam KV. Corticosteroids and glaucoma risk. Drugs Aging 1999; 15:439-50.
9. Gupta S, Sihota R, Gupta V, Dada T, Gogia V, Sharma A. Functional pituitary tumors masquerading as primary glaucoma and effect of hypophysectomy on intraocular tension. J Glaucoma 2015;24:e7-e13.
10. Spaeth GL, Idowu O, Seligsohn A, et al. The effects of iridotomy size and position on symptoms following laser peripheral iridotomy. J Glaucoma 2005; 14:364-7.
11. Ricardo JR, Medhi J, Pineda R. Femtosecond laser-assisted keratopigmentation for the management of visual disabilities due to peripheral iridectomies. J Glaucoma 2015;24:e22-e24. | |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in