|
|
 |
|
|
|
|
|
Bilateral retinochoroiditis in a case of acute primary toxoplasmosis in an immunocompetent patient
Digital Journal of Ophthalmology 2006
Volume 12, Number 2
December 28, 2006
|
Printer Friendly
|
|
|
|
|
| Abstract | Objective
To describe an uncommon case of an immunocompetent patient with bilateral retinochoroiditis due to acquired primary Toxoplasma gondii infection (atypical ocular toxoplasmosis).
Methods
Observational case report.
Results
A 46 year-old immunocompetent female presented with bilateral, acute toxoplasmosis, confirmed by elevated antibody titers. Systemic work-up for an underlying immune compromising disorder was negative. The patient’s vision improved with resolution of the inflammatory response after systemic treatment with pyrimethamine, sulfadiazine, and leucovorin.
Conclusion
Acquired Toxoplasma gondii infection should be considered in cases of bilateral retinochoroiditis in immunocompetent patients.
Keywords
acquired toxoplasmosis
atypical ocular lesion
bilateral retinochoroiditis
immunocompetent
ocular toxoplasmosis
primary toxoplasmosis
toxoplasma gondii
| | | Introduction | | Toxoplasma gondii is an uncommon cause of bilateral posterior uveitis occurring primarily in immunocompromised patients. To our knowledge no previous cases of bilateral retinochoroiditis due to acquired Toxoplasma gondii infection occurring in an immune competent patient have been reported. | | | Materials and Methods | | Report of a case. | | | Results | A 46-year-old female presented to our facility with the complaint of decreased central vision in her right eye for 3 weeks with concomitant myalgias, febrile episodes, night sweats, and chills. Her ocular history was significant for right orbital fracture with subsequent repair five years prior to presentation.
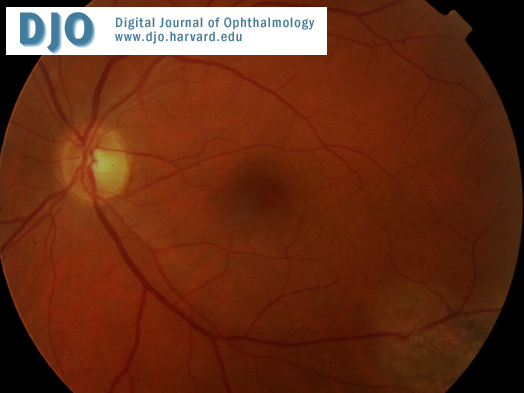
On examination, best-corrected vision was 20/60 OD and 20/20 OS. Slit-lamp examination revealed a bilateral posterior uveitis with spill-over into the anterior chamber. Dilated fundoscopic examination revealed a 2 disc diameter, elevated, creamy retinal lesion OD (Figure 1). A similar, yet smaller, patchy white lesion was noted OS (Figure 2). The patient was initially treated topically with 1% prednisolone acetate and 1% cyclopentolate, and an extensive hematologic work-up was initiated. Six days later vision had decreased to 20/400 OD and 20/40 OS, with significant enlargement of the retinal lesion OD.
A presumed diagnosis of toxoplasmosis was made on clinical appearance, and the patient was treated with intravitreal clindamycin and dexamethasone OD, along with oral Bactrim. A systemic work-up including tests for Toxoplasma gondii, tuberculosis, syphilis, Borellia burgdorferi, Bartonella henselae and quintana, HSV, HIV, ESR, ANCA, and ANA titers were processed to rule out infectious or inflammatory etiologies. Computed tomography imaging of the entire body and complete blood count with differential were also performed to evaluate for underlying lymphoma or possible metastatic disease. With the exception of elevated Toxoplasma IgM and IgG antibody titers, all studies were normal with no evidence of underlying immune suppressing disorder. Given the positive toxoplasmosis serologies with marked visual impairment, the patient was started on pyrimethamine, sulfadiazine, and leucovorin. Eight weeks after initiation of treatment, her visual acuity improved to 20/40 OD and 20/25 OS, with regression of the retinal lesions bilaterally (Figures 3 and 4).
| |

Figure 1
Right Fundus on presentation
|
|

Figure 2
Left Fundus on presentation
|
|

Figure 3
Right Fundus post-treatment
|
|

Figure 4
Left Fundus post-treatment
|
|
| Discussion | Ocular involvement reportedly is uncommon in immunocompetent individuals with acquired toxoplasmosis (1), unlike that seen with the congenital form. To our knowledge, no cases of acquired Toxoplasma gondii infection with bilateral ocular involvement in an immunocompetent patient have previously been reported. Bilateral retinochoroiditis is atypical and has previously only been described in congenital cases and in certain subgroups of patients—elderly persons, patients infected with human immunodeficiency virus, and patients with other forms of systemic immunosuppression.(2)
The classic indications for treatment of ocular toxoplasmosis include: 1) lesions located in the papillomacular area, 2) large retinal lesions (>2 disc diameters) with marked visual impairment, and 3) all lesions in immunocompromised patients. A wide variety of anti-parasitic therapies have been used, and the synergistic combination of pyrimethamine and sulfonamides is the classic and most common therapy.(3) In addition, reports have stated the benefit of concomitant intravitreal dexamethasone and clindamycin in reducing the ocular inflammation secondary to toxoplasmosis.(4, 5) In our patient, the use of both localized and systemic treatment affected regression of the retinal lesions with improvement of visual acuity. Acquired Toxoplasma gondii infection should be considered as a possible cause of bilateral posterior uveitis in immunocompetent patients, and we suggest that a more aggressive approach be applied to patients with atypical presentations with concomitant visual impairment. | | | References | 1) Masur H, Jones TC, Lempert JA, Cherubini TD. Outbreak of toxoplasmosis in a family and documentation of acquired retinochoroiditis. Am J Med 1978; 64(3): 396-402.
2) Smith JR, Cunningham ET. Atypical presentations of ocular toxoplasmosis. Current Opinion in Ophthalmology 2002; 13: 387-92.
3) Holland GN, Lewis KG. An update on current practices in the management of ocular toxoplasmosis. Am J Ophthalmol 2002;134(1): 102-14.
4) Martinez CE, Zhang D, Conway MD, Peyman GA. Successful management of ocular toxoplasmosis during pregnancy using combined intraocular clindamycin and dexamethasone with systemic sulfadiazine. Int Ophthalmol 1998-99; 22(2): 85-8.
5) Kishore K, Conway MD, Peyman GA. Intravitreal clindamycin and dexamethasone for toxoplasmic retinochoroiditis. Ophthalmic Surg Lasers 2001; 32(3): 183-92.
| | | Clinical Pictures | Figures 1 and 2. Patient with bilateral retinal lesions. (top) Color fundus photograph showing a 2 disc diameter elevated creamy, white lesion with fluffy borders OD, and (bottom) patchy white lesions OS.
Figures 3 and 4. Patient with bilateral resolution of lesions. Approximately 8 weeks after initiation of treatment, note the regression of the bilateral lesions OD (top) and OS (bottom).
| |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in