|
|
 |
|
|
|
|
|
Unilateral Superior Rectus Aplasia Without Craniofacial Anomaly
Digital Journal of Ophthalmology 2005
Volume 11, Number 5
October 12, 2005
|
Printer Friendly
|

Abbas Bagheri, M.D. | Shahid Beheshti University, Iran Ahmad Ferdosi | Dept. of Ophthalmology, Boston Medical Center Anne Bottros, M.D. | Dept. of Ophthalmology, Boston Medical Center David Hunter, M.D. | Dept. of Ophthalmology, Children's Hospital, Boston MA
|
|
|
| Abstract | Objective
To describe a rare case of unilateral superior rectus aplasia in a patient without craniofacial anomalies.
Methods
Observational case report.
Results
A 21 year old man presented with an incomitant left hypotropia of 35 prism diopters. Forced ductions were free. At surgery, the superior rectus muscle was absent. The patient responded to vertical transposition of the horizontal rectus muscles.
Conclusion
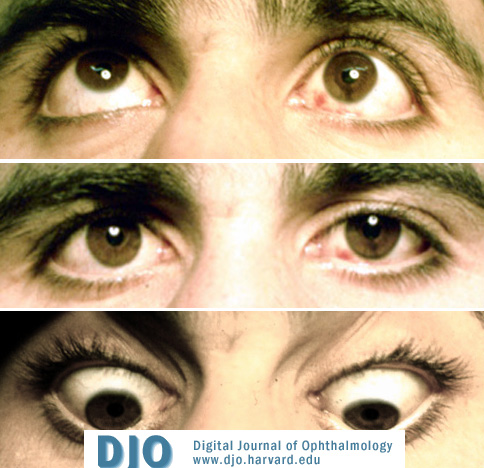
Rectus muscle aplasia should be considered as a possible cause of strabismus in congenital cases of incomitant strabismus, even in the absence of craniofacial anomalies. | | | Introduction | | A 21-year-old man presented to the Labbafinejad Hospital, Tehran, Iran, with the complaint of ocular misalignment since birth. There was no history of eye trauma or surgery and no family history of similar eye problems. He was the product of a normal vaginal delivery. | | | Materials and Methods | | Best-corrected visual acuity was 20/20 in the right eye and 20/30 in the left eye. There was 2 mm of pseudoptosis of the left eye. Motility testing revealed a 20 PD esotropia and 35 PD left hypotropia, increasing to 45 PD in up gaze and decreasing to 15 PD in down gaze (Figure 1). No A or V pattern was present. Elevation of the left eye both in abduction and adduction was limited to 25% of normal. Forced ductions were normal. Stereopsis was not detectable, and the Worth 4-dot test showed suppression of the left eye. Fundus torsion was not assessed. | |

Figure 1.
Pre-operative appearance. Top, upgaze; Middle, primary position; Bottom, downgaze.
|
|
| Results | | At surgery, the superior rectus muscle was absent (Figure 2.) A 180° superior limbal conjunctival incision was performed to improve visualization; despite extensive exploration posteriorly, no muscle tissue or other elastic tissue was identified. Anterior ciliary arteries were identified in the normal location of the superior rectus muscle. The superior oblique tendon fanned out temporally and its anterior border was 17.7 mm from the limbus. The horizontal rectus insertions appeared normal except for slight upward displacement. To correct the motility disorder, the horizontal rectus muscles were further transposed vertically, placing the inferior border 7.7 mm from the upper limbus, separated by 7 mm. Post-operatively, the vertical alignment improved but the esotropia had increased to 30 PD. Three months later, the left medial rectus was recessed 5 mm and the left lateral rectus resected 6 mm without altering the previous transposition. At the two-month post-operative visit, he was orthotropic in primary position, with 10 PD of left hypotropia in upgaze and 10 PD left hypertropia in down gaze (Figure 3). Diplopia in the reading position responded to 8 PD of prism added to the reading segments only. At the 15-month post-operative visit, he had stable alignment and no further complaints. Post-operative CT scan showed a decreased volume of the superior rectus-levator complex on the left (Figure 4). | |
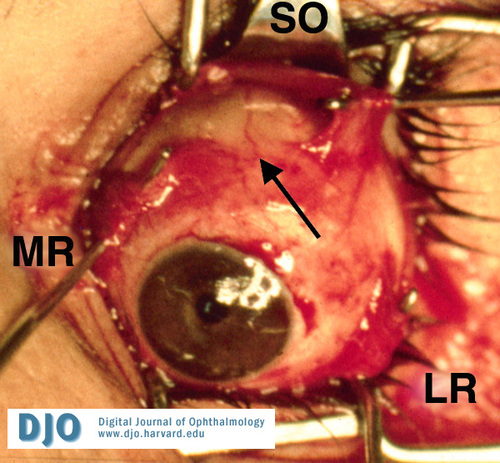
Figure 2.
Intraoperative photograph demonstrating absence of superior rectus. Muscle hooks are shown retracting the lateral rectus muscle, the medial rectus muscles and the superior oblique tendon. Arrow shows ciliary artery.
|
|
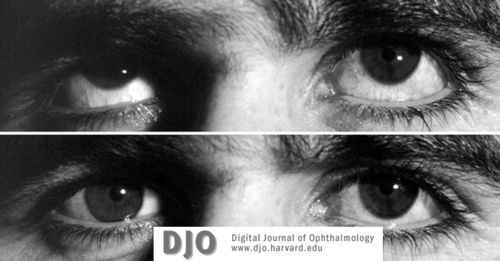
Figure 3.
Post-operative appearance. Top, upgaze. Middle, primary position; Bottom, downgaze.
|
|

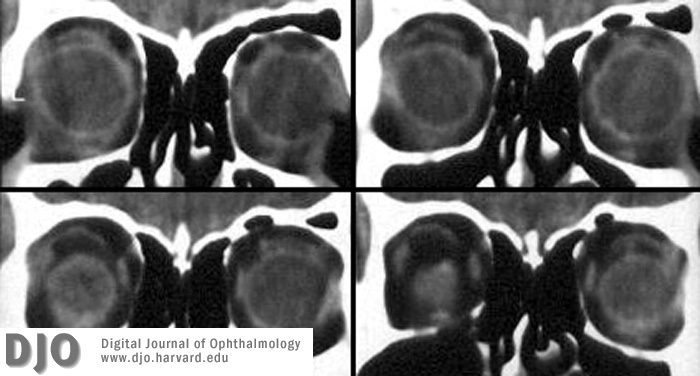
Figure 4.
CT scan demonstrating decreased volume of superior rectus-levator complex (four sequential coronal views).
|
|
| Discussion | | To our knowledge this is the first report of unilateral superior rectus aplasia without associated craniofacial anomaly. Hypoplasia and aplasia of superior rectus muscle have been reported in patients with craniofacial anomalies, most commonly Apert syndrome, Crouzon syndrome and Treacher-Collins syndrome.1-4 In one report of bilateral superior rectus aplasia without typical craniofacial anomaly, the patient had mild maxillary hypoplasia and anodontia that has been described as an atypical (or form fruste) craniofacial anomaly.5 Our patient had no craniofacial or systemic abnormalities. It is also remarkable that forced ductions were free, without secondary contracture of the inferior rectus muscle. Rectus muscle aplasia should be considered as a possible cause of strabismus in congenital cases of incomitant strabismus, even in the absence of craniofacial anomalies. | | | References | 1. Cuttone JM, Brazis PT, Miller MT, Folk ER. Absence of the superior rectus muscle in Apert’s syndrome. J Pediatr Ophthalmol Strabismus 1979; 16:349-54.
2. Snir M, Gilad E, Ben-Sira I. An unusual extraocular muscle anomaly in a patient with Crouzon’s disease. Br J Ophthalmology 1982; 66:253-7.
3. Diamond GR, Katowitz JA, Whitaker LA, Quinn GE, Schaffer DB. Variations in extraocular muscle number and structure in craniofacial dysostosis. Am J Ophthalmol 1980; 90:416-18.
4. Weinstock FJ, Hardesty HH. Absence of superior recti in craniofacial dysostosis. Arch Ophthalmol 1965; 74: 152.
5. Mather TR, Saunders R.A. Congenital absence of the superior rectus muscle: A case report. J Pediatr Ophthalmol Strabismus 1987; 24 (6): 291-5.
| |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in