|
|
 |
|
|
|
|
|
Aqueous shunt to the ocular surface for severe dry eye
Digital Journal of Ophthalmology 2005
Volume 11, Number 2
March 9, 2005
|
Printer Friendly
|

Claes Dohlman, M.D. | Massachusetts Eye and Ear Infirmary, Schepens Eye Research Institute, Harvard University Jan Dohlman, M.D. | East Boston Neighborhood Health Center, Boston University
|
|
|
| Abstract | Objective
In very dry eyes from any etiology, there is a need for near-continuous fluid supply to the ocular surface. Here is presented a patient with severe dry eyes who had a double-tubed valve shunt implanted to divert the aqueous humor to the lower lid fornix, thereby wetting the eye. Such arrangement has previously been used in eyes with keratoprosthesis and glaucoma.
Methods
A 67 year old woman had been severely incapacitated with pain and photophobia for many years. Tear menisci were virtually absent, Schirmer values were repeatedly zero, and vision was reduced in one eye. Etiology seemed to be scarring of lacrimal gland ductules caused by vernal catarrh.
Results
The shunt was implanted without complications, immediately resulting in wetting. After 6 months the eye is totally quiet and comfortable, with 20/25 vision and mild epiphora due to obstructed canaliculi. The tube in the lower fornix is rarely felt. Antibiotic drops are given twice daily and no infection has occurred.
Conclusion
So far the patient has done well with a totally quiet and wet eye. The only complication has been epiphora. If the long-term risks are low, this principle may be of value in end-stage dry eyes such as in autoimmune diseases, chemical burns, and trachoma.
Keywords
dry eye, aqueous shunt | | | Introduction | Very severe dry eyes without any visible tear secretion are common in chronic, end-stage inflammatory and scarring conditions of the ocular surface. Autoimmune diseases, such as ocular cicatricial pemphigoid (OCP), Stevens - Johnson syndrome (SJS), graft-versus-host disease (GVHD), as well as severe chemical burns, can end up with totally dry keratinized corneas. In addition, longstanding trachoma, vernal catarrh and other chronic inflammatory ocular surface conditions – common worldwide – can likewise lead to severe dryness. The cause of the surface dryness would be expected to be scar formation around the lacrimal ductules from the lacrimal gland and accessory glands, obstructing the flow from otherwise normal lacrimal gland tissue. This is in contrast to the much more common situation in e.g. Sjögren’s syndrome where the gland itself becomes inflamed and dysfunctional but where the tear secretion rarely ceases completely.
Therapeutic options to wet the ocular surface in the most severely dry eyes are few. The canaliculi have usually already scarred close, obstructing outflow. Tarsorrhaphy has limited value and scleral lenses are difficult to fit, expensive, and only rarely successful in the long run. This leaves artificial tear solutions as drops as the only practical alternative but with limited retention time and effectiveness. Treatment of the inflammatory component of the underlying disease has usually at this stage failed to prevent the final dryness. Therefore the possibility of providing a continuous flow of fluid over the ocular surface in dry eyes has intrigued ophthalmologists for decades. Thus spray pumps, attached to spectacle frames, have been developed with increasing sophistication(1,2). Also, pump systems leading fluid to the fornices via subcutaneously placed tubings have been tested (3-5). Transposition of salivary gland ducts to the lower lid fornix is surgically possible but the unevenness of the salivary secretion during the day has been a problem (6). Autotransplantation of submandibular gland is a more recent and promising approach (7).
Another principle for establishing continuous fluid delivery to the ocular surface could be the diversion of aqueous humor to the lid formices. Some recent developments in glaucoma shunt technology might accomplish such arrangement. Standard glaucoma shunt plates can become enclosed by a dense capsule, causing the intraocular pressure to rise to unacceptable levels. Diverting the aqueous humor to nearby epithelialized cavities where a fibrous capsule is less likely to form, has been shown to bypass the problem. Past research on this principle has included experiments in monkeys(8) and a patented device (9). More recently this concept has been tested in humans with severe glaucoma after keratoprosthesis surgery (10-12). Thus valved tube shunts have been implanted in patients, diverting the aqueous humor to a nasal sinus or to the lower lid fornix. Only one very recent infection has occurred in 32 such patients (8 with tubes to the fornix), with a follow-up time of up to 3 ½ years (cumulatively 54 shunt years). This development opens the possibility of using such valve shunts to the lid fornix in severe dry eyes as well. Here we describe the initial outcome of such a procedure in a patient who for many years has suffered from debilitating keratoconjunctivitis sicca.
| | | Materials and Methods | The patient is a 67 year old woman with a history of several decades of increasingly severe irritation in both eyes (Fig. 1). The diagnosis of dry eyes was made over 20 years ago. All puncta had been closed, the lower cauterized, and the upper had plugs. The patient was at the time of examination so incapacitated that she had to wear dark glasses and she used more than one bottle of artificial tears per day for instillation which still gave her only momentary relief. She was otherwise healthy and she had no symptoms of dry mouth or rheumatoid arthritis. On examination visual acuity was found to be 20/70 in the right eye and 20/20 in the left. Intraocular pressures were 8 and 10 mm Hg respectively, by applanation tonometry. Schirmer tests were repeatedly 0 mm/5 minutes, with anesthesia, in both eyes. Slit lamp examination revealed virtual absence of tear menisci (Fig 2). Fluorescein staining showed superficial punctate keratitis in the right cornea, less in the left.
Examination of the tarsal conjunctivae suggested the etiology of the condition. There was a whitish subepithelial sheen, indicating diffuse scarring from healed vernal conjunctivitis (difficult to photograph). On further questioning, the patient remembered severe eye problems for several years during her childhood.
The patient underwent examination by a rheumatologist (JGD). No history of systemic connective tissue disease could be elicited and the patient appeared healthy. Sedimentation rate was 15 mm, ANA screen negative, rheumatoid factor was normal, SS antigens negative. The hematological profile was normal. There was no history of dry mouth. On the basis of these findings, Sjögren’s syndrome appeared unlikely.
The possibility of implanting a valve shunt diverting aqueous to the lower lid fornix, thereby wetting the ocular surface, was discussed in detail with the patient who desired to have the operation done in her worse, right eye. Extensive informed consent for the operation was obtained preoperatively and the Institutional Review Board was consulted. The surgery consisted of implanting a valve shunt which had been manufactured at our request by New World Medical, Inc. (Rancho Cucamonga, CA). The shunt, previously described (11,12), consists of a proximal fine tube of silicone to be inserted to the anterior chamber. It connects to a valve similar to that of a standard Ahmed S-2 valve shunt, made for an opening pressure of 10 – 12 mmHg. Our shunt did not have a plate but rather the valve was enclosed by a silicone rubber housing. From the side of this housing a distal tube emerges to be drawn up to the lower lid fornix (Fig. 3).
The proximal tube to the anterior chamber was inserted beneath a half-depth 4 mm scleral flap, entering into the anterior chamber through a 23 g needle track of the limbus. The tube extended approximately 3 to 4 mm into the anterior chamber and was positioned anterior to the iris (Fig. 4). The valve housing was sutured to the sclera in the lower nasal quadrant with two 9-0 nylon sutures, in a manner similar to the attachment of a standard S-2 shunt plate. The distal tube was tied to a 4-0 silk suture and the needle was passed temporally under the conjunctiva to about midpoint of the fornix where it was exited upwards, and the tube was pulled through. The tube was cut so that it was allowed to lie flat in the fornix, extending for about one centimeter. Two 10-0 nylon sutures were placed to temporarily keep the tube flat at the bottom of the fornix. Aqueous could immediately be seen trickling out of the tube opening. A soft contact lens (Kontur 16.0 mm diameter, 9.8 mm base curve, plano, Kontur Kontact Lens Co, Inc., Richmond, CA 94801) was finally placed on the eye. It was kept for 2 weeks in order to keep the patient more comfortable.
| |

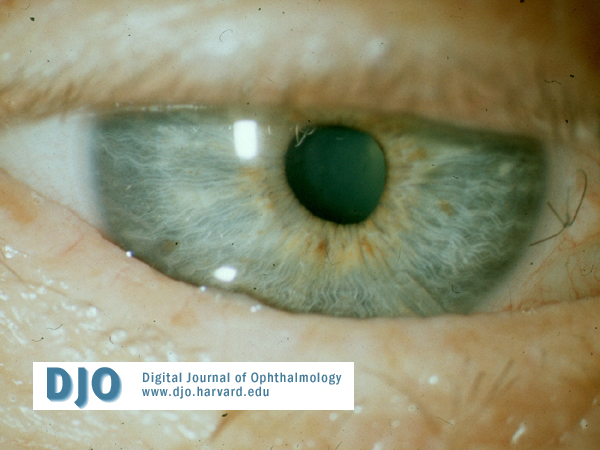
Figure 1.
67-year old female with many years of marked discomfort from very dry eyes.
|
|

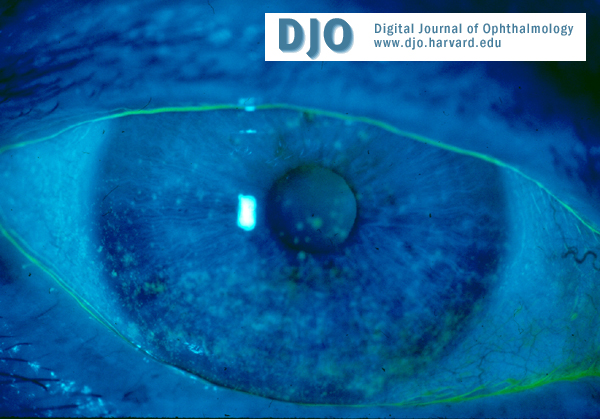
Figure 2.
Virtual absence of tear menisci (fluorescein staining). Schirmer values repeatedly 0 mm /5 minutes. Superficial punctate keratitis. Vision 20/70.
|
|

Figure 3.
Valved tube shunt. The short tube is inserted into the anterior chamber. The valve is totally enclosed in silicone rubber and is attached to the sclera in the lower nasal quadrant. The long tube is drawn temporally through the conjunctiva, shortened and left at the bottom of the lower lid fornix. Aqueous is then delivered continuously to the fornix and distributed over the surface of the eye by blinking.
|
|

Figure 4.
Post-operative appearance. Since puncta and canaliculi had been obliterated earlier, the lower lid tear meniscus is voluminous and there is mild epiphora. The corneal epithelium has healed and the vision is restored. The intraocular tube is visible in the 5 o’clock meridian.
|
|

Figure 5.
The distal tube is visible at the bottom of the lower lid fornix where it is rarely felt. The eye is quiet and there is no conjunctival reaction.
|
|
| Results | Postoperatively the patient did well with a minimum discomfort for a few days. In fact, she felt instantaneous relief when the lower tear meniscus welled up (Fig. 4). She reported occasional epiphora (the puncta had been left closed). Schirmer tests postoperatively varied from 5 mm to 17 mm in 5 minutes, with anesthesia. After one month visual acuity had increased to 20/25. The intraocular pressure has been measured at between 5 mm and 9.5 mm by applanation tonometry. There has been no shallowing of the anterior chamber, hypotony maculopathy, or other complications of hypotony.
The patient initially received vancomycin (14 mg/ml), moxifloxacin 0.5 % and prednisolone acelate 1 %, all topically four times daily. This regimen was over a month lowered to twice a day. Three weeks postoperatively an attempt was made to open the right upper punctum to relieve the epiphora. Dissection under local anesthesia by an ophthalmic plastic surgeon, Dr. Peter Rubin, resulted in removal of the plug stem but the caniliculus remained scarred and obliterated. A re-canalization procedure is planned for the future.
Later in the minor operating room under topical anesthesia, the tube was shortened to about 5 mm exposed length. An additional 10-0 nylon suture was placed to keep the tube at the bottom of the fornix (Fig. 5). The patient has during the follow-up period of 6 months felt substantial relief in the operated eye and she is, so far, satisfied with the outcome.
| | | Discussion | The encouraging aspect of this patient’s short-term follow-up is not only that the aqueous humor wets the external eye surface so well but also that the eye rapidly became very quiet without irritation. The relief was almost instantaneous after the operation. Also, the exit tube is very rarely felt at the bottom of the lower lid fornix, only if the eye is rubbed. This was expected from our experience with fluid delivery via a subcutaneous tube to the lower lid fornix(3,4).
The only, fortunately minor, side effect has been epiphora, due to the obliterated canaliculi. In severely dry eyes, such as in end-stage autoimmune diseases, the puncti and canaliculi are usually completely scarred down. Surgical recanalization is very difficult in these cases and epiphora may be the price to pay for the continuous wetting of the eye. On the other hand, if the canaliculi are open, it has been our experience that glaucoma patients with fornix shunt do not report epiphora during the day. Occasionally they describe “some wetness on the pillow” when they wake up in the morning. This is probably explained by the fact that aqueous is secreted continuously around the clock (2 uL/min(13)). Tear production during the day has similar value but the night-time secretion is markedly reduced (14). Thus the slight epiphora during the night is likely due to uninterrupted aqueous secretion and absence of blink pump during sleeping hours.
What are the potential long-term risks in this technique of diverting aqueous to the lid fornix? First, there must be the usual risks of glaucoma shunts such as tube or valve erosion and exposure, intraocular tube damage to the corneal endothelium, intraocular obstruction of the tube, or, rarely, infection. Then the added risk of infection due to the connection with the conjunctival surface must be considered. However, based on previous experience with valve shunts ending in the nasal sinuses or lower lid fornix, the risk of endophthalmitis seems low. In more than 50 cumulative shunt years only one recent infection has occurred. These valved tube shunts seem to have unidirectional flow, thus fluid cannot in vitro be forced from the distal end to exit through the proximal tube opening. It is unlikely that the low dose prophylactic antibiotics (vancomycin plus a fluoroquinolone once or twice a day) which are given routinely after keratoprosthesis (with or without shunt), could prevent infection if a bacterial bolus managed to reach the inside of the eye. This suggests that it is the unidirectional flow of the aqueous that reduces the risk of infection.
There could still be the risk of infection around the stoma in the conjunctiva where the distal tube exits into the fornix. After all, the normal conjunctiva is the host of a number of bacteria such as Staphylococcus epidermidis and Corynebacteria species, as well as Haemophilus, Moraxella, Proprionobacterium acnes, etc (15). Again no infection has occurred in the tissues around the tube exit in altogether 9 cases of valve shunt to the lower fornix, followed for up to 20 months. Here it is quite possible that the routinely given topical antibiotics do manage to suppress bacterial colonization and infection. Clearly a future step in the development of this shunt-to-fornix method will have to be trying to minimize use of antibiotics.
The described principle of wetting the ocular surface with aqueous is technically feasible. It may find some application in the end-stage autoimmune diseases where epithelial inflammation may be the basis for the disease process but where lack of fluid may also play a large role.
| | | Acknowledgements | Presented at the International Symposium on Lacrimal Gland, Tear Film, and Dry Eyes 4, held in Puerto Rico November 2004.
Supported by a grant from Alcon Research Institute.
Corresponding author:
Claes H. Dohlman, M.D., Ph.D
Massachusetts Eye and Ear Infirmary
243 Charles Street
Boston, MA 02114
Tel: (617)573-3240
Fax: (617)573-4369
Email: Claes_Dohlman@meei.harvard.edu
| | | References | 1. Flynn F, Schulmeister A: Keratoconjunctivitis Sicca and new techniques in its management, Med J Austral 1967; 1:33-41
2. Bertera JH, Dohlman CH, Ma JK Programmable microdroplet dispenser functions as an artificial lacrimal gland. (ARVO abstract). Invest Ophthalmol Vis Sci 2003;2451.
3. Dohlman CH, Doane MG, Reshmi CS: Mobile infusion pumps for continuous delivery of fluid and therapeutic agents to the eye. Ann Ophthalmol 1971;3:126-128
4. Ralph RA, Doane MG, Dohlman CH. Clinical experience with a mobile ocular perfusion pump. Arch Ophthalmol 1975;93:1039-43.
5. Murube J, Murube E, Chen Zhou L, Rivas L: Subcutaneous abdominal artificial tears pump -reservoir for severe dry eye. Orbit 2003;22:29-40
6. Bennett JE, Bailey AL. A surgical approach to total xerophthalmia. Transplantation of the parotid duct to the inferior cul-de-sac. Arch Ophthalmol 1957;58:367-71.
7. Geerling G, Sieg P, Bastian GO, Laqua H. Transplantation of the autologous submandibular gland for most severe cases of keratoconjunctivitis sicca. Ophthalmology 1998;105:327-35.
8. Camras CB, Wang RF, Siegel MJ, et al. Valved tube shunt from the anterior chamber to the external ocular surface for use in refractory glaucoma. Invest Ophthalmol Vis Sci 1992;33:3949. (ARVO abstract).
9. White TC. US Patent 082837, 1989.
10. Dohlman CH, Grosskreutz CL, Dudenhoefer EJ, Rubin PAD: Can a glaucoma shunt be safely extended to the lacrimal sac or ethmoid sinuses in keratoprosthesis patients? Preliminary findings. Dig J Ophthalmol 2002;7:3
11. Dohlman CH, Barnes SD, Ma JJK, et al : Diverting aqueous humor to distant sites in severe glaucoma: an update. Invest Ophthalmol Vis Sci 2004 (ARVO)
12. Dohlman CH, Barnes SD, Ma JJK, et al. Diverting aqueous humor to epithelialized cavities in severe glaucoma. Submitted.
13. Sears ML: The Aqueous. In: Adler’s Physiology of the Eye (Moses RA, ed) St Louis, CV Mosby Company 1981;p.204
14. Baum JF: Clinical implications of basal tear flow. In: The Preocular Tear Film in Health, Disease and Contact Lens Wear (Holly FJ, ed); Dry Eye Institute, Lubbock TX 1986; p.646
15. Perkins R, Kundsin RB, Pratt M, et al: Bacteriology of normal and infected conjunctiva. J Clin Microbiol 1975; 1:147
| |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in