|
|
 |
|
|
|
|
|
The Use of Standard Thin High Water Content Artificial Iris and Black Pupil Contact Lenses
Digital Journal of Ophthalmology 2001
Volume 7, Number 1
March 1, 2001
|
Printer Friendly
|
 John de Brabander Optom MSc, Cor
John de Brabander Optom MSc, Cor | Eye Research Institute Maastricht J van Mil Optom BSc | Eye Research Institute Maastricht, University of Maastricht, The Netherlands and Medical Center at the University of Amsterdam, Oculenti practice, Amsterdam, The Netherlands Cees J J Brinkman MD PhD | Eye Research Institute Maastricht, University of Maastricht, The Netherlands and Medical Center at the University of Amsterdam, Oculenti practice, Amsterdam, The Netherlands R.M.M.A. Nuyts MD PhD | Eye Research Institute Maastricht, University of Maastricht, The Netherlands and Medical Center at the University of Amsterdam, Oculenti practice, Amsterdam, The Netherlands
|
|
|
| Abstract | Objective
Fitting prosthetic contact lenses with artificial irises and so-called "black pupils" can be problematic due to low water content materials, thick lens designs, and the loss of color with time. In particular black pupil lenses often do not provide adequate occlusion. Furthermore, delivery times are long and it is difficult to produce the lenses such that the color of the other eye is matched to the patients satisfaction. The aim of this study was to evaluate whether the use of standardized lenses would ease prosthetic lens fitting.
Methods
In this study, 34 eyes of 31 patients were fitted with thin, high water content standardized soft contact lenses. The lenses were available in 5 standard colors with opaque iris posterior surfaces and a printed iris pattern on the anterior surface. Iris and pupil diameters are standardized to 12.5 and 5 mm, respectively. Black occluding pupils are available in diameters FROM 5 to 10 mm in 1 mm steps.
Results
In 67% of eyes, the selected standard color of the lens was satisfactory to the patient. In 78% of the eyes the standard lens dimensions could be used. No adverse physiological reaction of the eyes was noticed during the one year follow-up. The iris prosthetic and black pupil lenses proved at the dispensing visit to be adequately opaque and/or totally occluding in all cases. Loss of color was, in 71% of the eyes, a reason to REPLACE lenses between 4 to 8 months after dispensing (average 6.5 months).
Conclusion
The thin high water content standardized prosthetic lenses as used in this study provided success in 67% of the cases.
Keywords
Artificial iris; black-pupil; occlusion; prosthetic soft contact lenses | | | Introduction | Hydrophilic contact lenses, with their large diameters and good centering properties, are ideal in cases where an artificial iris or occluding black pupil is indicated. There are two types of prosthetic soft lenses available [1,2]. The heterogeneous type has a laminated construction whereby a printed or hand painted iris shield is sandwiched between two HEMA sections. With these lenses all iris patterns and colors can be created but their disadvantages are cost, long delivery time, poor reproducibility and very poor oxygen transmissibility [3]. The second available type is called homogeneous because a normal hydrophilic lens is colored using a dyeing process. The advantages are that one can use thin, high water content lenses [4] in a large range of colors at a relative low price and acceptable delivery time [5]. With these lenses, problems reported are the lack of a sufficient opaque layer and an unnatural look when using a heavy coloring without iris pattern. With black pupil lenses patients often report that the occlusion in not total or that there is still hindering light entering the eye via the borders of the artificial black pupil. Several manufacturers have made attempts to improve the dying technique or, by the addition of an iris pattern, give the lenses a more natural look.
One of the presently available systems is subject of this study. Next to the use of a high water content material and all possible fitting parameters, the idea behind this system is to use a limited amount of colors and standardize the dimensions of iris and pupil. The aim of this study is to evaluate the clinical performance and success-rate of this system in cases where an artificial iris with clear or black pupil or a black pupil only is indicated. | | | Materials and Methods | The study was open to patients with ocular conditions that indicated the use of iris prosthetic or occluding black pupil contact lenses. After obtaining oral informed consent FROM the patient, a routine ophthalmological examination was performed. Using a slit lamp measuring eye-piece, the horizontal diameter of iris and pupil was determined. In case the iris was not visible the horizontal corneal diameter was measured. K-readings were taken whenever possible and thereafter lenses were fitted according to the instruction of the manufacturer. If no K-readings could be obtained the fitting was done on basis of trial and error. For later reference a color slide was made of each and both eyes, with and without contact lenses.
All lenses were produced FROM a non-ionic random co-polymer based on N-Vinyl 2-pyrrolidone HAVING a water content of 67.5 %. The production of the lenses involved a color dyed within the lens matrix (homogeneous type), an additional opaque backing and an iris pattern printed on the anterior surface. The individual lens color was selected FROM a trial set containing the five available standard colors. Standard dimension of the iris was 12.5 mm with a pupil diameter of 5 mm. The system, Prosthetic Hi-colour SELECT manufactured by Igel International (Igel, Leighton Buzzard, UK) offers the option of a clear and black pupil combined with the prosthetic iris. Also available is a clear lens with a black dot, in diameter ranging FROM 5 to 10 mm, to be used as a black occluding pupil.
At the dispensing visit the lenses were placed on the patient eye(s) and evaluated with standard procedures for fitting of soft contact lenses. The patients were instructed on care and handling of the lenses. The care system used was Unicare blue (ICN, Zoetermeer, The Netherlands), extra wetting of the lens was allowed whenever needed but solely by using unit dose NaCl 0.9%.
Follow up visits were routinely scheduled at 6 weeks, 3, 6 months and one year after dispensing. Patients were entitled to extra visits in case adverse reactions or subjective disturbing symptoms were noticed. At initial and each follow up visit the system was evaluated using following criteria. Good fit is formulated as movement of 0.5 to 1.0 mm on the blink and centering such that the edge of the lens extends minimal 0.5 mm over the limbus in any direction including movement. Success of the lens was evaluated using the patients subjective findings in daily use and the objective examination of iris and pupil coverage. Corneal physiology was assessed and recorded following the standard procedures (CCLRU) as described by Terry [6] for soft contact lenses under daily wear conditions. Loss of color over time was checked by observing the visibility of the iris or the corneal tissue behind the lens in situ using the slitlamp beam as a light source. The observations were scored on a 5 point scale representing 0, 25, 50, 75 or 100% loss of color. The criteria for lens replacement were 50% loss of color or patient subjective dissatisfaction wit the opaqueness of the lens. | | | Results | A total of 31 patients (18 females, 13 males, 34 eyes), with ocular conditions that indicated the use of an artificial iris and/or occluding black pupil, were included in this study. The age of the patients ranged FROM 14 to 67 years of age (average 38.4 years of age). FROM the 34 eyes fitted, 17 needed a prosthetic iris/clear pupil, 9 a prosthetic iris/black pupil and 8 a black pupil only. In TABLE 1 the indications and the type of lens used are given.
Although the combination and the severity of signs and symptoms varied considerably among patients three main areas of indication for this type of lenses could be deduced. The first GROUP consisted of various types of iris defects with photophobia, nystagmus, glare and hinder of incident light as signs and symptoms. In the second GROUP lenses were fitted for cosmetic reasons in non functioning eyes due to severe pathology or trauma. The third GROUP represented cases in which (binocular) vision was permanently disturbed, therapy had failed and only occlusion remained to relief diplopia.
Figure 1 shows an example of a case in GROUP one (iris defects) indicating the use of a lens with an artificial iris and clear pupil. Figure 2 is an example of an artificial iris and a black pupil used for GROUP 2 problems (cosmetic). An example of indication area 3 (disturbed vision) is given in figure 3. The lens used had a black pupil only, with the special condition that it is also used as a bandage in a case of trichiasis.
In 78 % of the eyes the standard dimensions of iris and pupil could be used. In 67 % of the cases that needed a lens monocularly, one of the standard iris colors matched the fellow eye to the patients satisfaction. The opaqueness of the prosthetic iris and the occlusion of the black pupil lenses proved at the dispensing visit to be satisfactory in all cases.
No adverse reactions were seen during the one year follow-up. The only reason for patients to appoint for extra follow ups was discoloration of the lenses and subsequent returning of subjective symptoms. In combination with the criteria to REPLACE lenses if 50% loss of color was observed this resulted in 71 % of the cases to REPLACE the lens in a range between 4 to 8 months (average at 6.5 months) after dispensing.
Two patients wear their lenses occasionally and one was discontinued due to lack of motivation.
Conclusion
The standard available high water content Prosthetic Hi-Colour SELECT contact lenses could be used successfully in cases where an iris prosthesis and/or a black pupil is indicated. Color matching showed to be satisfactory in 67 % of the cases. Discoloration and loss of opacity was in 71% of the cases a reason to REPLACE the lenses at average 6.5 months after dispensing. This study shows that homogeneous colored thin high water content lenses can be successfully used as a first choice option in prosthetic contact lens fitting. | | | Discussion | The results of our study indicate that in a systematic evaluation of cosmetic fitting in traumatized eyes, it is efficient, FROM a physiological standpoint, to first try standardized thin high water content colored soft lenses. With this study we can therefore conform this type of hypothesis FROM case reports [2,4].
The use of standardized colors seems to be in accordance with the report of Golightly [5] on tinted contact lenses for non-traumatized eyes. With a limited choice of options in color it was found that patients are more easily satisfied than with the promise of exactly matching the color of the other eye as offered in hand-painted lenses.
Loss of color over time is the most important problem we have seen with this type of lenses. Loss of color varies considerably among patients. In 29% of the cases the same lens still performed satisfactory after one year whereas in other cases the lens needed replacement as early as 4 months after dispensing. It was noticed that, although with some variation, the frequency of required replacement seems to be patient related. Since all patients used the same care system (without mechanical cleaning) the reason for loss of color and the variations per patient must either be found in differences in tear composition, in variations in washing out of the dye FROM the lens matrix, or maybe in the variation with which patient used artificial tears.
With the tendency of early replacement in soft contact lens wear to avoid complications in general the replacement problem is in our view only a matter of management. Information about color loss of the lenses to the patient, and the insurance company prior to the dispensing avoids problems in cost management of lens replacements. | | | Acknowledgements | | We thank ICN/Oculenti and Igel International for their support in this study. | | | References | 1. Port, M. Cosmetic and prosthetic contact lenses. Contact Lenses, chapter 21:p789-95, edited by Phillips AJ and Stone J. London, Butterworths, 1989.
2. Stechler, J. Fitting traumatised eyes with tinted and hand-painted hydrogel lenses. Optician 201; part1; 5299; part2; 5304:8-29 (1991).
3. Holden, B.A. and Mertz, G.W. Critical oxygen levels to avoid corneal edema for daily and extended wear contact lenses. Invest Ophthalmol Vis Sci 25:1161-71 (1984).
4. Goede, H. Die Anpassung einer hoch hydrofhilen getoenten Kontaktlinse wegen aesthetischer Indikation. DOZ 10:106-7 (1991).
5. Golightly, C. How To Fit Colored Lenses More Efficiently. Contact Lens Forum 18: 49-53 (1990).
6. Terry, R.L. et al. CCLRU standards for success of daily and extended wear contact lenses. Optom Vis Sci 70:234-43 (1993). | | | Tables |
HEIGHT="312">
|
Indications |
Iris prosthetic clear pupil |
Iris prosthetic black pupil |
Black pupil |
Traumatic iris defect |
5 |
|
|
Iridectomy |
3 |
|
|
Iris pigment defects |
3 |
|
|
Iris coloboma |
2 |
|
|
Albino |
2 |
|
|
Aniridia |
2 |
|
|
Corneal scar |
|
2 |
3 |
Corneal decompensation |
|
5 |
|
Diplopia |
|
1 |
4 |
Non-functioning eye |
|
1 |
1 |
Total |
17 |
9 |
8 |
| | | Clinical Pictures | | | |

Figure 1
Photographic documentation of a patient with iris coloboma. Top left shows the condition of the (OD) eye to correct. Bottom left shows OD with the prosthetic lens. Top right shows OD and OS without (top) and with corrective lens (bottom).
|
|

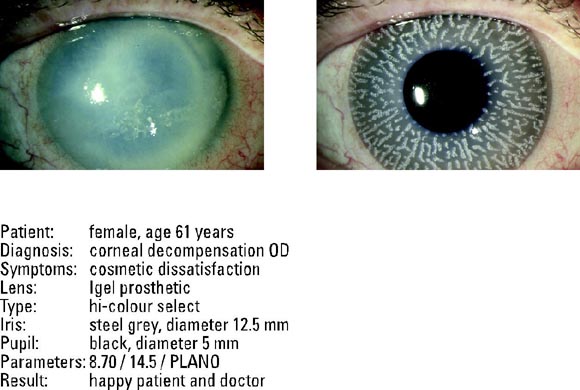
Figure 2
Photographic documentation of a patient with corneal decompensation OD. Top left shows the condition of the (OD) eye to correct. Top right shows OD with the prosthetic lens. The legend gives details on the case.
|
|
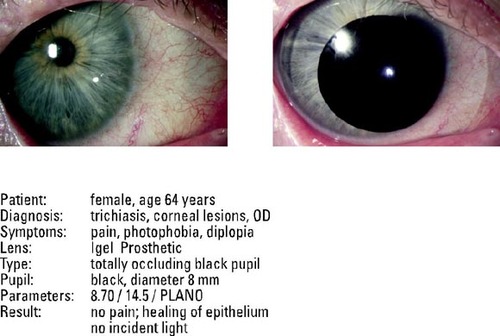
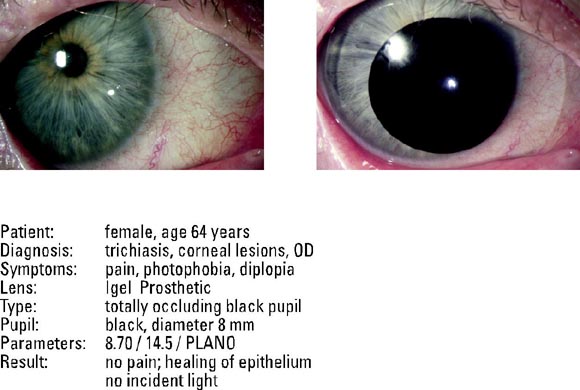
Figure 3
Photographic documentation of a patient with diplopia and trichiasis OD. Top left shows the condition of the (OD) eye to correct. Top right shows OD with the occlusion lens. The legend gives details on the case.
|
|
|
|
 Welcome, please sign in
Welcome, please sign in