|
|
 |
|
|
|
|
|
Boston Keratoprosthesis in Stevens-Johnson syndrome: a case of using infliximab to prevent tissue necrosis
Digital Journal of Ophthalmology 2009
Volume 15, Number 1
February 20, 2009
|
Printer Friendly
Download PDF |

Jan G. Dohlman, MD | East Boston Neighborhood Health Center, East Boston, MA, USA C. Stephen Foster, MD | Massachusetts Eye Research and Surgery Institute, Cambridge, MA and Harvard Medical School, Boston, MA, USA Claes H. Dohlman, MD, PhD | Massachusetts Eye and Ear Infirmary, Boston, MA and Harvard Medical School, Boston, MA, USA
|
|
|
| Abstract | Purpose: To report the case of a patient with Stevens-Johnson Syndrome (SJS) with Boston Keratoprosthesis (KPro) who may have benefited from infliximab infusions.
Materials and Methods:
Patient A 34-year-old woman with a history of acute SJS at age 12 had three Boston KPro Type II implanted since 2003 into her right eye. The first two were followed by tissue necrosis and aqueous leak, necessitating reoperation. After the third device was implanted, monthly infliximab infusions were started.
Methods Infliximab 5 mg/kg infusions were started in January 2008, repeated after 2 weeks, and then given monthly for a year. The treatment is continuing combined with regular eye examinations.
Results: While receiving infliximab, the skin around the keratoprosthesis has not shown a trace of retraction or necrosis. This is in sharp contrast to events following the two previous attempts at visual rehabilitation. The patient’s vision has been generally stable for a year and is currently 20/30.
Conclusion: A KPro in a patient with SJS normally has a poor long-term prognosis. However, retention of the prosthesis and visual outcome may benefit from monthly infliximab infusions. | | | Introduction | Recent developments in the field of keratoprosthesis (design, case selection, postoperative management) have led to substantial improvements in the treatment of patients with severe corneal diseases. In cases in which standard corneal transplantation has failed repeatedly or in which such transplantation has been deemed hopeless to begin with, a Boston KPro has had considerable success in restoring vision.(1)
However, of all disease categories needing a KPro, autoimmune diseases such as Stevens-Johnson Syndrome (SJS), ocular cicatricial pemphigoid (OCP), graft-versus-host disease, and uveitis have the poorest prognosis.(2) Typically, following a KPro in end stage SJS, vision is good for a few months, or a year or two, but chronic postoperative inflammation can result in media opacities, retroprosthetic membrane, epiretinal membrane or cystoid macular edema (CME). If the Type II device is used, as in the case reported here, the covering lid skin typically retracts from the KPro nub and the front plate, leading to surrounding tissue necrosis, ulceration and even perforation.(3) Retinal detachment is a common postoperative occurrence in SJS (Jardeleza MSR, Montezuma SR, Dohlman CH, Young L. Retinal detachment after Boston Keratoprosthesis: incidence, predisposing factors and outcomes of repair. ARVO abstract 2009). The risk of bacterial endophthalmitis is now small after the advent of topical vancomycin prophylaxis,(4) but the incidence of glaucoma is still high.(5) These complications seem to be the consequence of the high propensity for inflammation in SJS, easily triggered by KPro surgery even in its quiet stage. In our experience, corticosteroids have proved to be a double-edged sword in that tissue melt and perforation can result from its use, even in low doses. It therefore seems logical to look further for means of suppression of the inflammation, whether it is immunologically mediated or not.
TNF-alpha antagonists are widely used in many severe chronic inflammatory conditions and have been employed, off-label, in isolated non-ocular manifestations of toxic epidermal necrolysis (a variant of SJS) with some encouraging results.(6) They have also been used with success in treating uveitis.(7,8) Topical soluble tumor necrosis factor receptor has been found to suppress corneal transplant rejection in mice.(9) However, use in connection with the KPro in SJS has not been previously attempted to our knowledge. In this report, we describe a case with two consecutive failures followed by a successful third attempt in the setting of monthly infusions of the anti-TNF-alpha antibody infliximab. | | | Materials and Methods | Case report
The patient is a 34-year-old Asian female with a history of severe SJS at the age of 12, contracted after a viral infection while living in South Korea. One year later, she had a Seoul-type keratoprosthesis implanted in the left eye. Six months later, the eye developed a retinal detachment which could not be repaired at the time.
At the age of 19, the patient moved to Boston, MA, USA. Since the left eye still had light perception vision, an attempt was made in 1993 to repair the KPro eye by performing a vitrectomy and a scleral buckle. The surgery was a functional failure and the eye went blind shortly afterwards.
In the meantime, the right eye was followed closely. In 1993 a superficial keratectomy was attempted, but it had no beneficial effect (Figure 1). However, special attention was given to the intraocular pressure, which was grossly estimated as normal by finger palpation throughout her course. In 2003 the patient expressed strong interest in having a Boston-type KPro in this eye. She was told that the long-term prognosis for a KPro in SJS was still highly uncertain and that a cosmetically questionable through-the-lid Type II KPro would have to be used. Also, due to the likelihood of severe glaucoma developing after surgery, she was advised to have a glaucoma shunt implanted first. In May 2003 a special valve shunt was implanted which directed the aqueous humor to the maxillary sinus.(10) This was successful and in July 2003 the KPro Type II implantation was performed using previously described techniques.(1) Also, the crystalline lens was removed and therefore aphakic correction was chosen for the KPro.
The immediate postoperative course was successful (Figure 2), and the visual acuity reached 20/20 within one month. Prophylactic antibiotic drops were instituted for indefinite use: vancomycin 14 mg/ml and moxifloxacin 0.3%, both twice daily. No topical steroids were given.
The intraocular pressure (IOP), as measured by finger palpation, rose suddenly after 3 months necessitating the implantation of an additional shunt, a standard Ahmed S-2 valve shunt. This brought the pressure to a normal level.
Also, within a few months after the KPro implantation, signs of skin necrosis and retraction away from the nub appeared although there was no leak at this stage. A retroprosthesis membrane formation required opening with YAG laser twice, one month and sixteen months postoperatively. Vision was restored to the 20/30 range, and the intraocular pressure was normal.
In February 2006, the patient had a major aqueous leak. The lid skin had retracted to the edge of the front plate and necrosis had led to a fistula. Vision was still 20/70. A reoperation with a fresh graft and KPro Type II plus anterior vitrectomy was performed without complications. A temporary complete tarsorrhaphy was done. There was a suspicion of fungal colonization and therefore voriconazole 200 mg twice daily was instituted. Two weeks later the tarsorrhaphy was opened around the KPro nub. No fungal infection was found and anti-fungal medication was stopped. The visual acuity was 20/60, and improved to 20/30 two weeks later.
Slow skin retraction gradually set in again after the second KPro surgery, and it had become clinically obvious within a year. A crust formed over the naked plate. The visual acuity was 20/20. However, in October 2007 the patient noted “foggy vision.” The visual acuity was 20/40, but the IOP had dropped to less than 5 mm Hg. No leak could be detected.
In December 2007, the visual acuity was down to 20/200. YAG laser was used to break up vitreous membranes around the shunt tube. A sub-tenon injection of 40 mg triamcinolone was given after the laser treatment. There was little visual improvement.
Ten days later the patient noticed a definite leak (Figure 3). A third KPro Type II operation was performed. At this stage the future course was reconsidered. The skin around the nub had retracted and resulted in necrosis and leak in the first two attempts and the third KPro was expected to be heading in the same direction. In addition, B-scan ultrasound showed macular elevation, consistent with cystoid macular edema (CME). Optical Coherence Tomography (OCT) for confirmation could not be used at this stage due to vitreous haze. It was decided to start treating the patient with the TNF-alpha antibody infliximab.
The third Boston Keratoprosthesis was similarly a Type II with a nub that protrudes through the lid skin.(1) The surgery was performed in December 2007 by CHD, and it followed previously established surgical guidelines.(1) Before starting the infliximab (Remicade, Centocor) infusions, the patient was thoroughly evaluated for possible contraindications. Following the guidelines, no signs of acute infection were found. There was no history of recurring infections, history of TB or exposure to TB, chronic obstructive pulmonary disease, hematologic or liver diseases, demyelinating diseases, seizure disorder, heart disease, lymphoma or skin cancer. She had no other medical problems beyond her SJS sequelae. A PPD skin test was negative.
The patient had her first infusion with infliximab 5 mg/kg over 3 hours on January 18, 2008, supervised by CSF. There was no adverse reaction. The next infusion followed two weeks later and thereafter on a monthly basis. The treatment is still ongoing.
Periodic laboratory tests, consisting of complete blood count and hepatic enzyme measurements, were done. They were all normal. Standard ophthalmological examinations were conducted every month. They usually included photography and occasionally OCT. | |

Figure 1
The right eye of a 34-year old patient with a history of SJS. Vision in the opposite eye had been lost.
|
|

Figure 2
A through-the-lid Boston KPro Type II was performed in 2003. The photo shows the situation one month postoperatively. The initial result was good but later tissue necrosis and leak necessitated re-operation.
|
|

Figure 3
The second KPro resulted in skin retraction, necrosis, melt and leak thus requiring repeat surgery. The crust partially obscures the retracted skin.
|
|
| Results | Three weeks following the first Remicade infusion, vision had reached 20/60. There was a thin retroprosthetic membrane, which was opened with YAG laser followed by a sub-Tenon's injection of 40 mg triamcinolone. Two weeks later vision was 20/40.
In March 2008 the media had cleared enough to allow a reliable OCT examination, which showed cystic changes in the macula with a thickness of 565 microns and a slight epiretinal membrane. The patient continued to be followed on a monthly basis. In August 2008 she developed a mild sudden vitritis without pain or redness.(11) It was presumed to be sterile and was treated with a short burst of systemic prednisone (60 mg, rapidly tapered over one month). The cystoid macular edema had remained stationary.
The most remarkable feature at present is the health of the skin around the KPro nub (Figure 4). It has a perfectly normal and uninflamed texture without any edge retraction or necrosis. It encloses the nub firmly. Also, the media are very clear and the vision is better than 20/30. No side effects of the infliximab have occurred besides a very slight fatigue during the first month. | |

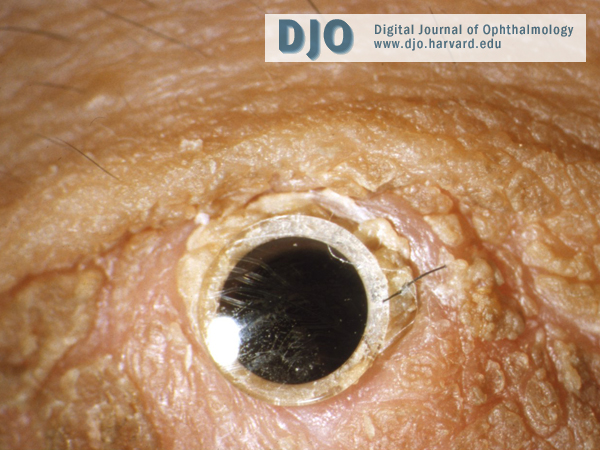
Figure 4
At the time of the third KPro Type II, the patient was started on infliximab infusions which are still continuing. More than a year postoperatively the lid skin around the nub is remarkably intact and free from inflammation and necrosis, the media are clear and vision is 20/30.
|
|
| Discussion | After KPro implantation in an eye of a SJS patient, it might be expected that postoperative corticosteroids should be useful in preventing any longstanding inflammation and its possible consequences. Unfortunately, it has been our experience that topical or systemic steroids have little effect on the inflammation in this circumstance and instead contribute to rapid tissue melt and leak around the KPro. Non-steroidal anti-inflammatory drugs can also have a melt-provoking effect.
Standard immunomodulating medications such as Dapsone, methotrexate or cyclophosphamide have been tried in KPro situations where SJS activity has flared up with uncertain results in our hands. Due to the present lack of understanding of the pathogenesis and tissue cytology in SJS, we are left to try anti-inflammatory approaches in an empiric way. There are a number of biological avenues to be tested such as immunoglobulins, TNF-alpha inhibitors, B-cell inhibitors, and other newer immunomodulators. We have used infliximab in a SJS patient with repeated tissue melts in the past, and it may have contributed to the rather dramatic initial results. We have earlier shown extraordinary improvement after infliximab infusions for KPro patients in cases of severe rheumatoid arthritis,(12) but the biological situation is most likely different in SJS. Nevertheless, the patient described here has encouraged us to continue, despite the cost and potential risk, to explore the possible long-term benefits of infliximab in SJS patients with KPro. | | | Acknowledgements | Supported by Massachusetts Eye and Ear Infirmary Keratoprosthesis Fund.
This review has adhered to the tenets of the Declaration of Helsinki. Informed consent was obtained for all invasive procedures and infusions. The patient was educated about the infliximab and its off-label use. | | | References | 1. Dohlman CH, Nouri M. Keratoprosthesis surgery. In: Foster CS, Azar D, Dohlman CH, eds. Smolin and Thoft’s The Cornea 4th ed. Philadelphia: Lippincott, Williams and Wilkins, 2005;1085-1095
2. Yaghouti F, Nouri M, Al-Merjan J, et al. Keratoprosthesis: Preoperative prognostic categories. Cornea 2001;20:19-23
3. Sayegh RR, Ang LPK, Foster CS, Dohlman CH. The Boston Keratoprosthesis in Stevens-Johnson Syndrome. Am J Ophthalmol 2008;145:438-44.
4. Durand ML, Dohlman CH. Successful prevention of bacterial endophthalmitis in eyes with the Boston Keratoprosthesis. Cornea, in press.
5. Netland PA, Terada H, Dohlman CH. Glaucoma associated with keratoprosthesis. Ophthalmology 1998;105:751-57.
6. Fisher M, Fiedler E, Marsch WC, Wohlrab J. Antitumour necrosis factor-alpha antibodies (infliximab) in the treatment of a patient with toxic epidermal necrolysis. Br J Dermatol 2002;146:707-709.
7. Joseph A, Raj D, Dua HS, et al. Infliximab in the treatment of refractory posterior uveitis. Ophthalmology 2003;110:1449-53.
8. Suhler EB, Smith JR, Wertheim MS, et al. A prospective trial of infliximab therapy for refractory uveitis: preliminary safety and efficacy outcomes. Arch Ophthalmol 2005;123:903-12.
9. Qian Y, Dekaris I, Yamagami S, Dana MR. Topical soluble tumor necrosis factor receptor type I suppresses ocular chemochine gene expression and rejection of allogeneic corneal transplants. Arch Ophthalmol 2000;118:1666-71.
10. Dohlman CH, Grosskreutz CL, Chen TC, Pasquale LR, et al. Shunts to divert aqueous humor to distant epithelialized cavities after keratoprosthesis surgery. Glaucoma, in press.
11. Nouri M, Durand ML, Dohlman CH. Sudden reversible vitritis after keratoprosthesis: an immune phenomenon? Cornea 2005;24:915-19.
12. Dohlman CH, Dudenhoefer EJ, Khan BF, Dohlman JG. Corneal blindness from end-stage Sjögren’s Syndrome and Graft-vs-Host Disease. In: Sullivan D, ed. Lacrimal Gland, Tear Film and Dry Eye Syndrome III Adv Exp Med Biol. New York: Plenum Publishing, 2002. | |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in