|
|
|
Register
with DJO to receive personalized updates.
If you're already a
member, please sign in.
|
|
|
|
|
|
|
|
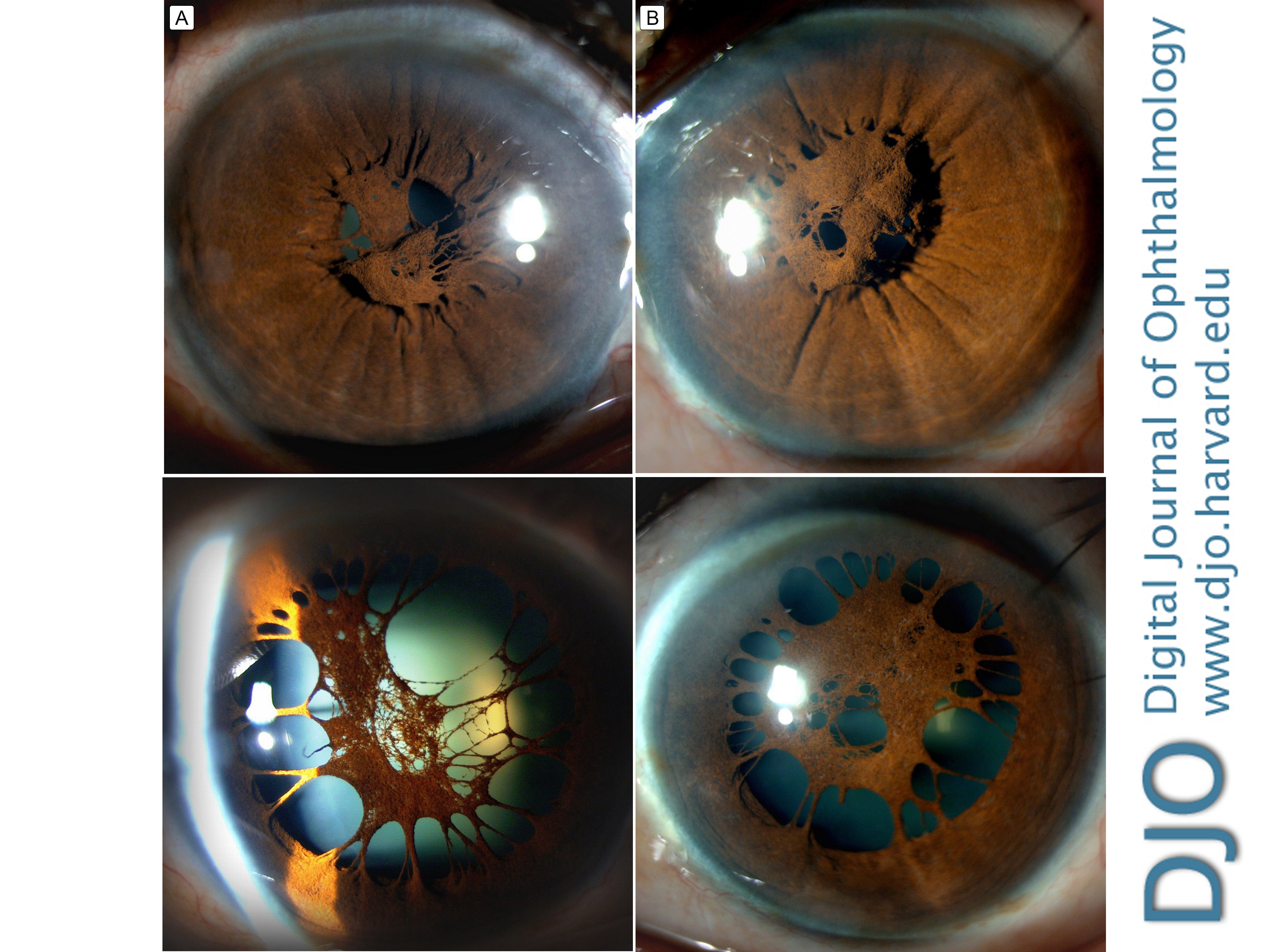
Accessory iris membrane Sep 5, 2021 Volume 27, Number 3 Sudhakar Potti, MS | Department of Cornea and Refractive Surgery, Sankara Eye Hospital, Guntur, Andhra Pradesh, India Aparna N. Nayak, MBBS, MS, DNB, FICO | Department of Cornea and Refractive Surgery, Sankara Eye Hospital Guntur, Andhra Pradesh, India  A 54-year-old woman presented at Sankara Eye Hospital, Guntur, Andhra Pradesh, with poor vision in both the eyes from the age of 2 years. She had been using mydriatics on and off for many years. She discontinued the medications a few months before presenting at our institution for evaluation. On examination, best-corrected visual acuity was 6/24 in the right eye and 3/60 in the left eye. The corneas were clear, and the anterior chambers were quiet. The pupils were reactive, with dense strands of iris tissue attached to the collarette and a central pseudopupil in both eyes that was not reactive to light. The figure shows slit-lamp photography of the undilated (top) and dilated (bottom) pupil with pseudopupil of the left eye (A) and right eye (B). Age-related nuclear sclerosis was noted, worse in the left eye. Fundus examination was unremarkable. The patient was diagnosed with accessory iris membrane (AIM), with cataract, and offered pupilloplasty with cataract extraction. AIM, or “iris duplication,” is a rare congenital ocular anomaly, with a similar origin to persistent pupillary membrane (PPM) but differing in appearance. AIM shows iris tissue strands arising from the collarette and resembles the normal iris in thickness and color, with a pseudopupil in the center and no associated muscular activity. PPM, on the other hand, has fine strands of iris, with transclusent or opaque membrane across the pupil, remnants of tunica vasculosa lentis, which supplies nutrition to the lens in the first 6 months of fetal life; size, density, and configuration vary. A pupil diameter of 1.5 mm is required for retinal image formation, and AIM is rarely associated with dense amblyopia. If visual acuity is good, the condition can be managed medically with mydriatics; Nd-YAG laser may be used to clear the visual axis. Membranectomy may be required for dense AIM. |
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in