|
|
|
Register
with DJO to receive personalized updates.
If you're already a
member, please sign in.
|
|
|
|
|
|
|
|
Scleral melt following mitomycin-C application after pterygium excision Nov 18, 2019 Volume 25, Number 4 Akhil Bevara, DNB Ophthalmology | Sankara Eye Hospital, Guntur, Andhra Pradesh, India Shashidhar Banigallapati, MS Ophthalmology | Sankara Eye Hospital, Guntur, Andhra Pradesh, India 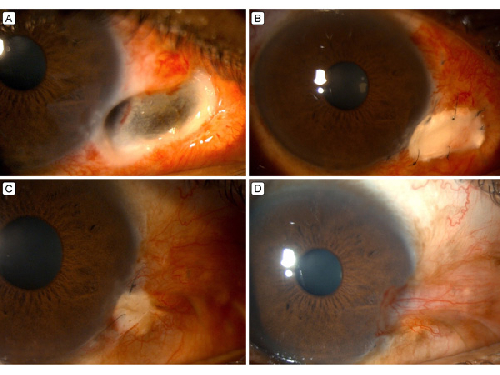 A 38-year-old man underwent pterygium excision in the right eye using a bare sclera technique with application of mitomycin C to the scleral bed intraoperatively 1 month before presenting at the Sankara Eye Hospital, Guntur, India, with a scleral melt measuring 5 × 3 mm and involving almost the full thickness of the sclera, including the limbus inferonasally at the site of pterygium excision (A). Scleral patch graft was advised, and an allogenic donor patch graft conforming to the dimensions of the melt was sutured to the surrounding sclera using 10-0 nylon sutures (B). An amniotic membrane graft was placed over the entire area of pterygium excision. Topical and systemic steroids were prescribed in tapering doses along with topical antibiotics and lubricants. The scleral graft was healthy at the 1-month follow-up examination (C), and the scleral surface healed completely by 6 months (D). Scleral thinning, melt, and necrotizing scleritis are uncommon complications of topical mitomycin C in pterygium excision. Preferably, low doses of mitomycin C should be used after pterygium excision, and the scleral bed should be thoroughly washed of any remnants of the drug with at least 30 ml of balanced salt solution. If a scleral melt occurs, it must be treated aggressively medically or, in severe cases, surgically to prevent globe perforation. |
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in