|
|
 |
|
|
|
|
|
A 51-year-old woman with binocular diplopia and unilateral ptosis
Digital Journal of Ophthalmology 2019
Volume 25, Number 3
August 18, 2019
|
Printer Friendly
Download PDF |
|
|

Landon J. Rohowetz, BS | University of Missouri – Kansas City School of Medicine, Kansas City, Missouri Anjulie K. Quick, MD | Department of Ophthalmology, University of Kansas School of Medicine, Prairie Village, Kansas
|
|
|
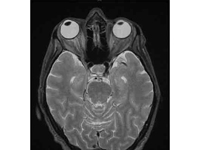
| Ancillary Testing | A complete blood count revealed anemia, with a hemoglobin concentration of 11 g/dL, but platelet and white blood cell counts were within normal limits. Electrolytes and coagulation studies were also within normal limits. With findings consistent with oculomotor nerve palsy, the patient was managed with the intent to urgently rule out aneurysm. Immediate computed tomography angiogram (CTA) of the head and neck was ordered, followed by magnetic resonance imaging (MRI), with and without contrast, of the head and orbits. CTA was unremarkable. T2-weighted MRI revealed mild right-sided proptosis and slightly increased cerebrospinal fluid (CSF) signal surrounding the right optic nerve but no abnormal enhancement and no mass or retrobulbar inflammation (Figure 2).
Lumbar puncture for CSF analysis revealed a normal opening pressure (15 cm H2O) and elevated concentrations of glucose (103 mg/dL) and protein (58 mg/dL). White blood cell count was within normal limits and differential analysis revealed 25% monocytes and 47% blasts. Gram stain, culture, fungal studies, and viral studies were negative. Flow cytometry revealed 41% myeloid blasts, consistent with relapse of AML. The following day, bone marrow biopsy was performed, revealing no bone marrow involvement.
| |
|
Figure 2
T2-weighted magnetic resonance imaging demonstrating mild right-sided proptosis and slightly increased cerebrospinal fluid signal surrounding the right optic nerve but no abnormal enhancement and no mass or retrobulbar inflammation.
 |
|
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in 


