|
|
 |
|
|
|
|
|
Multimodal imaging of type 2 acute macular neuroretinopathy in a young woman
Digital Journal of Ophthalmology
2021
Volume 27, Number 3
August 5, 2021
|
Printer Friendly
Download PDF |
|
|

James H. Powers, MD | Department of Ophthalmology, Duke University Medical Center, Durham, North Carolina Pali P. Singh, BS | Department of Ophthalmology, Duke University Medical Center, Durham, North Carolina Dilraj S. Grewal, MD | Department of Ophthalmology, Duke University Medical Center, Durham, North Carolina John D. Matthews, MD | Triad Retina and Diabetic Eye Center, Greensboro, North Carolina Sharon Fekrat, MD | Department of Ophthalmology, Duke University Medical Center, Durham, North Carolina
|
|
|
| Abstract | | We report a case of type 2 acute macular neuroretinopathy (AMN) that occurred in an otherwise healthy 22-year-old white woman taking oral contraceptives and consuming large quantities of caffeinated coffee. The patient presented with a teardrop-shaped scotoma just inferior to her central vision in her left eye after a recent and significant increase in coffee consumption. A small extrafoveal retinal lesion was present superior to the fovea on pseudocolor fundus photography. Multimodal retinal imaging demonstrated focal disruption of the inner segment-outer segment junction of the photoreceptors with overlying hyperreflectivity at the level of the outer plexiform layer superior to the fovea, consistent with a diagnosis of type 2 AMN. Oral contraceptive use and high caffeine intake may be risk factors for the development of type 2 AMN. | | | Introduction | Acute macular neuroretinopathy (AMN) is an uncommon condition characterized by the sudden onset of a paracentral scotoma(s), which may be associated with blurred vision, floaters, and metamorphopsia.(1) Although its microvascular pathogenesis is not completely understood, the condition is characterized by a highly distinctive wedge-shaped lesion on infrared or pseudocolor fundus photography as well as inner segment–outer segment junction abnormalities demonstrated on spectral domain optical coherence tomography (SD-OCT).(2) Some individuals experience partial improvement of the scotoma, but full resolution has not been reported previously. Risk factors include a febrile illness, viral infection, oral contraceptives, epinephrine/ephedrine, and systemic shock, while some less commonly associated factors include intravenous contrast exposure, pre-eclampsia, postpartum hypotension, and caffeine consumption.(3) Currently, no particular treatment of AMN has been shown to be beneficial.
AMN is often classified as type 1 or 2 based on the location of the primary lesion on OCT. Type 1 AMN, or paracentral acute middle maculopathy (PAMM), involves the inner retina, with OCT hyperreflectivity superficial to the outer plexiform layer (OPL) and potential thinning of the inner nuclear layer (INL). Type 2 AMN involves the outer retina, with associated hyperreflectivity deep to the OPL and potential thinning of the outer nuclear layer.(3) Type 1 AMN predominantly occurs in older men with an underlying vasculopathy, whereas type 2 AMN is typically reported in young, healthy white women.(4) | | | Case Report | A 22-year-old white woman with history of depression and allergic rhinitis initially presented to her local ophthalmologist 1 month after a teardrop-shaped scotoma appeared inferior to the central vision in her left eye. Multicolor imaging revealed a reddish-brown extrafoveal lesion superior to the fovea on pseudocolor and corresponding dark lesion on infrared imaging (Figure 1). Two months prior to scotoma onset, the patient experienced allergic symptoms resulting in chemotic and itchy conjunctiva, for which she was prescribed oral montelukast, leading to resolution of symptoms. The patient denied use of alkyl nitrite inhalants (ie, “poppers”) and any direct exposure to the sun or laser light. Family history was noncontributory. Review of symptoms was negative for other symptoms, illnesses, or remote travel. Other oral medications included norgestimate and ethinyl estradiol contraception (Sprintec, Teva Pharmaceuticals, Tel Aviv, Israel), which the patient had been taking for 2 years, and sertraline. The patient also reported that she had dramatically increased her caffeine intake in the weeks prior to symptom onset.
Corrected visual acuity was 20/20 in each eye. Slit-lamp examination of the anterior segment of both eyes was unremarkable. Ophthalmoscopy of both eyes was normal, and the lesion was not readily visible in the left eye. It was also not visible on ultra-widefield fundus photography (Figure 2A). On fluorescein angiography, there was subtle patchy blockage of fluorescence superior to the fovea and corresponding to the lesion’s location (Figure 2B). OCT revealed a focal extrafoveal hyperreflectivity of the outer plexiform layer (Figure 3), consistent with type 2 AMN. After the initial visit, the patient was lost to follow-up. | |

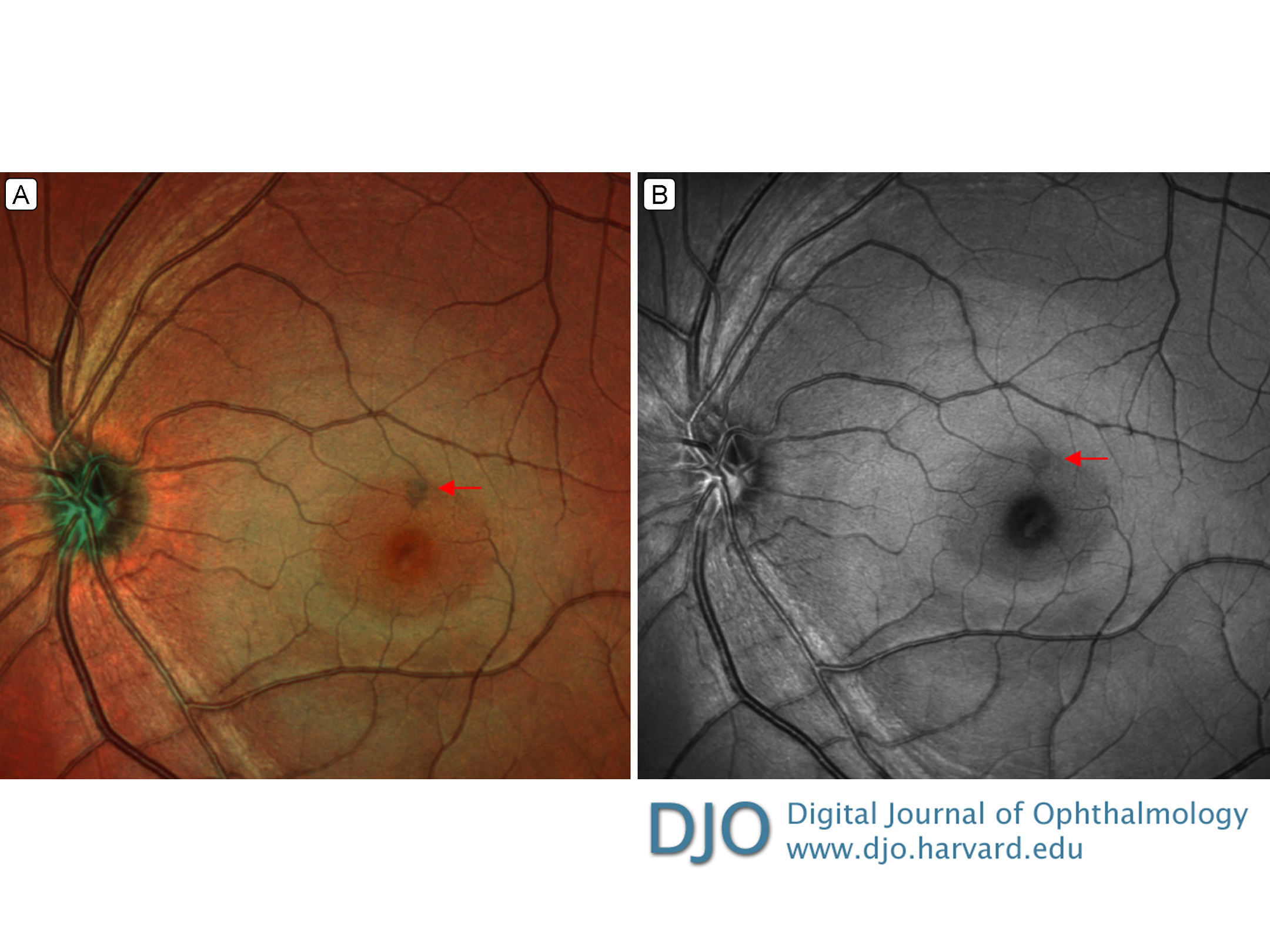
Figure 1.
Heidelberg multicolor (A) and red-free (B) images of left eye 1 month after symptom onset showing an extrafoveal retinal lesion superior to the fovea. Photo credit: Daryl Barber.
|
|

Figure 2.
A, Cropped ultra-widefield color photograph; the extrafoveal retinal lesion superior to fovea was not visible. The bright diagonal line inferior to the macula is an artifact. B, Fluorescein angiography demonstrating subtle patchy blocked fluorescence superior to the fovea corresponding to the lesion’s location. Photo credit: Daryl Barber.
|
|

Figure 3.
Vertical (A) and horizontal (B) spectral domain optical coherence tomography of left eye showing the focal hyperreflective extrafoveal lesion of outer plexiform layer superior to fovea. There is some focal photoreceptor loss (arrow).
|
|
| Discussion | We report a case of type 2 AMN in a young, otherwise healthy woman. Although uncommon, type 1 AMN typically occurs in older men with an underlying vasculopathy, whereas type 2 AMN occurs in younger, otherwise healthy females.(4) Our patient had two risk factors for the development of AMN: oral contraceptive use and increased caffeine intake.
Imaging findings made other causes of acute parafoveal scotoma less likely, including acute retinal pigment epithelitis, where the hyper-reflective lesion is mainly located at the photoreceptor outer segment layer as opposed to the plaques present at the border of the OPL and outer nuclear layer as seen in AMN.(5) Similarly, OCT findings were not indicative of other focal retinitis, which typically involves several retinal layers, and infectious testing, including toxoplasmosis, was negative.
Although the underlying pathogenesis of AMN is not well understood, an ischemic etiology has been hypothesized.(3) It has been theorized that focal occlusion of the retinal microvasculature in the superficial capillary plexus in the innermost portion of the INL in type 1 AMN or of the deep capillary plexus of the outermost portion of the INL in type 2 AMN leads to the development of the characteristic lesions.(6) This may be evident on OCT angiography.(7) Furthermore, the known risk factors of AMN predispose to vasoconstrictive and/or hypercoagulable states, suggesting an underlying ischemic etiology. It remains unclear exactly why older males typically present more commonly with type 1 AMN, whereas younger females most often present with type 2 AMN.
This case serves as a reminder for physicians to consider AMN in the differential diagnosis of individuals who present at any age with sudden-onset parafoveal scotoma. This report adds to the growing body of evidence that oral contraceptive use and high caffeine consumption may serve as risk factors for the development of AMN.
Literature Search
PubMed was searched on June 1, 2021 (restricted to the past 10 years), for English-language results, using the following terms: acute macular retinopathy AND type 2.
Declaration of conflicting interests
SF receives patent royalties from Alcon. DSG receives patent royalties from Alimera and Allergan. | | | References | 1. Dasingani KK, Freund KB. Paracentral acute middle maculopathy and acute macular neuroretinopathy: related and distinct entities. Am J Ophthalmol 2015;160:1-3.e2.
2. Lee SY, Cheng JL, Gehrs KM, et al. Choroidal features of acute macular neuroretinopathy via optical coherence tomography angiography and correlation with serial multimodal imaging. JAMA Ophthalmol 2017;135:1177-83.
3. Bhavsar KV, Lin S, Rahimy E, et al. Acute macular neuroretinopathy: a comprehensive review of the literature. Surv Ophthalmol 2016; 61:538-65.
4. Tsui I, Sarraf D. Paracentral acute middle maculopathy and acute macular neuroretinopathy. Ophthalmic Surg Lasers Imaging Retina 2013;44(6 Suppl):S33-5.
5. Iu LPL, Lee R, Fan MCY, Lam WC, Chang RT, Wong IYH. Serial spectral-domain optical coherence tomography findings in acute retinal pigment epitheliitis and the correlation to visual acuity. Ophthalmol 2017;124:903-9.
6. Sarraf D, Rahimy E, Fawzi AA, et al. Paracentral acute middle maculopathy: a new variant of acute macular neuroretinopathy associated with retinal capillary ischemia. JAMA Ophthalmol 2013;131:1275-87.
7. Casalino G, Arrigo A, Romano F, Munk MR, Bandello F, Parodi MB. Acute macular neuroretinopathy: pathogenetic insights from optical coherence tomography angiography. Br J Ophthalmol 2019;103:410-4.
| |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in