Late dislocation of the capsular bag–intraocular lens–modified capsular tension ring complex after knotless transscleral suturing using 9-0 polypropylene
Digital Journal of Ophthalmology
2020 Volume 26, Number 2 June 26, 2020 DOI: 10.5693/djo.02.2020.04.001
Natalia S. Anisimova, MD, PhD | A. I. Yevdokimov Moscow State University of Medicine and Dentistry, Moscow, Russia Lisa B. Arbisser, MD | John A. Moran Eye Center, University of Utah, Salt Lake City Natalya F. Shilova, MD, PhD | S. Fyodorov Eye Microsurgery Institution, Moscow, Russia Roman V. Kirtaev | Moscow Institute of Physics and Technology, Dolgoprudny, Russia Daria A. Dibina, MD | S. Fyodorov Eye Microsurgery Institution, Moscow, Russia Boris E. Malyugin, MD, PhD | A. I. Yevdokimov Moscow State University of Medicine and Dentistry, Moscow, Russia; S. Fyodorov Eye Microsurgery Institution, Moscow, Russia
We report a case of late breakage of a 9-0 polypropylene transscleral suture used for fixation of a dislocated capsular bag–intraocular lens–modified capsular tension ring complex in a 52-year-old woman with Marfan syndrome. Breakage occurred despite use of a cow-hitch technique for external and internal fixation. We believe breakage was caused by the suture chafing on the sharp edges of the modified capsular tension ring eyelet. Cross-sectional analysis of Malyugin-modified capsular tension rings from two different manufacturers revealed a difference with respect to radius of curvature. Suturing intraocular implants with relatively sharp edges may cause suture breakage; further studies are needed to identify the critical parameters for the surface quality of sutured intraocular implants.
Lack of zonular support, lenticular dysgenesis, and aphakia are common issues in anterior segment surgery that require intraocular lens (IOL) fixation. Commonly preferred surgical techniques for IOL centration and stabilization include both sutured and sutureless methods. Although, whenever possible, optic capture is optimal, when the bag cannot be employed, intra- and transscleral implant fixation as well as iris fixation techniques are available. Selection of the best procedure for any individual case depends on surgeon proficiency, familiarity with techniques, and the prevailing conditions in the eye. Polypropylene suture is approved for ophthalmic use and for intraocular implant fixation. Examples of suture failure are well recognized, but currently, there is limited evidence in the literature with regard to its exact etiology. Breakage of 10-0 polypropylene suture associated with superficial biodegradation is documented.(1) Additionally, the sharp edge of the IOL can traumatize the polypropylene material by chaffing.(2) As a result of these reports, many surgeons have turned to larger caliber (9-0 and 8-0) polypropylene (Prolene, Ethicon, Somerville, NJ), expecting improved long-term outcomes. The only single trial to date reporting long-term outcomes of 8 pediatric cases sutured with 9-0 Prolene, however, did not provide a detailed description of its single case of suture breakage.(3)
Both the type of suture material and the selection of surgical technique is important. Many authors extol the advantages of knotless Z-suturing fixation of the distal suture(4) and, for the proximal end, sliding knots, cow-hitch, or other modifications.(5-9) To date, however, there are no long-term results reported for the simultaneous use of these two techniques with either 9-0 or 8-0 polypropylene suture.
A 52-year-old woman with Marfan syndrome presented at S. Fyodorov Eye Microsurgery Institution with decreased vision in her left eye. She had undergone cataract surgery 5 years before in the right eye and 6 years before in the left with a Malyugin-modified capsular tension ring (MCTR) transclerally fixed with 9-0 polypropylene suture bilaterally. Both eyes were pseudophakic. On examination, best-corrected visual acuity was 20/25 in the right eye and 20/50 in the left eye. Intraocular pressure was within normal limits in each eye. Axial length measured 25.97 mm in the right eye and 25.83 mm in the left eye. Corneal topography showed stable with-the-rule and against-the-rule corneal astigmatism, in the right and left eyes, respectively, with cylinder of 0.63 in the right eye and 0.91 in the left eye in the 3.0 mm zone (flat keratometry [K] 43.66 @104, steep K 44.29 @ 14 and flat [K] 43.21 @173, steep K 44.12 @83).
Slit-lamp examination revealed a quiet anterior segment in the left eye, with no signs of scleral suture extrusion; however, the capsular bag–IOL-MCTR complex was subluxated in the inferior temporal direction (Figure 1). The superior zonules were absent, without vitreous prolapse. Fundus examination showed myopic conus on both sides but no retinal degeneration or other abnormalities.
Primary Surgery
Recorded video of the primary surgery and protocol were reviewed (Video 1). During surgery, prolapsed vitreous was eliminated by means of a triamcinolone-visualized “dry” automated vitrectomy. The anterior chamber was filled with a highly dispersive ophthalmic viscosurgical device (chondroitin sulfate–sodium hyaluronate 3%). A 7.0 mm Malyugin ring 2.0 (Microsurgical Technology Inc, Redmond, WA) was injected into the anterior chamber for iris expansion and transposition of the pupil in the direction of the dislocated crystalline lens. The continuous curvilinear capsulorhexis was initiated with a sharp cystotome, and a capsule retractor (MicroSurgical Technology Inc, Redmond, WA) was placed behind the leading edge of the tear for stabilization. A temporal fornix-based conjunctival flap was dissected to expose the sclera. A Malyugin-modified capsular tension ring (MCTR; Reper-NN, Nyzhny Novgorod, Russia) was placed into an inserter, and a single-armed 9-0 polypropylene loop-suture (MANI 1486L; Ideta Eye Hospital, Kumamoto City, Japan) was used to perform a cow-hitch knot through the leading eyelet outside the globe. The MCTR was then placed through the main incision into the capsular bag. With the fixation hook on the anterior capsule rim, the MCTR was dialed toward the area of missed zonules using a bimanual technique with no tension placed on the suture. The swaged suture needle was then passed through the paracentesis, located 180° from the area of dehiscence, keeping it above the capsulorhexis edge, emerging through the sclera in the area of the ciliary sulcus about 1.3 mm from the limbus. After the needle was externalized, the suture was affixed to the superficial scleral layers in a zig-zag fashion with 4-5 passes and secured using a double knot. After removal of the capsule retractor, multiple-quadrant hydrodissection was gently performed in a cortical cleaving fashion. Phacoemulsification with low-irrigation pressure was performed, and cortex material was removed. A foldable monofocal hydrophilic acrylic IOL (PhysIOL SA, Liège, Belgium) was implanted into the capsular bag. The pupillary expander Malyugin ring 2.0 was removed with an inserter. Finally, the ophthalmic viscosurgical device was washed out, and the incisions were hydrated. At the end of surgery, a stable central position of the capsular bag–IOL-MCTR complex had been achieved.
The immediate postoperative period was uneventful. Four years postoperatively, uncorrected visual acuity in the left was 20/40, correcting to 20/20 with refraction of −1.25 −0.5 ×5. At 5 years’ follow-up, the patient experienced acute deterioration of vision in her left eye, with best-corrected visual acuity having decreased to 20/50. On slit-lamp examination, dislocation of the capsular bag–IOL-MCTR complex was evident, accompanied by severe iridodonesis and a tendency of the complex to dislocate to the posterior segment in upgaze. Insufficient capsular support and complete loss of suture fixation was evident. There was no history of ocular or head trauma.
Refixation Surgery
Informed consent was obtained after explaining benefits, risks, and the investigative nature of the repeat surgery. Surgery was performed under topical and intracameral anesthesia (Video 2). Briefly, two clear corneal incisions were made (8 and 11 o’clock hours). Subsequently, the anterior chamber was filled with dispersive ophthalmic viscosurgical device (sodium hyaluronate 3.0%/chondroitin sulfate 4.0% [Viscoat; Alcon Inc, Fort Worth, TX]), and the two iris retractors were placed to dilate the pupil. Fornix-based conjunctival flaps were made inferior and temporally to the original fixation site and superior and nasally to the site of missed zonules. Additionally, two clear corneal paracenteses were performed at 4 and 10 o’clock. The needle of a 9-0 polypropylene loop suture (MANI 1486L) was passed through the paracentesis at 4 o’clock under the MCTR and pulled out through the opposite paracentesis. It was then returned through the same paracentesis, inserted through the suture loop, forming a cow-hitch knot, and externalized through the sclera. The iris retractors were removed, and Z-suturing was performed. The broken suture was subsequently identified in the inferior-temporal site and removed without noticeable resistance. The repeated suture was then placed at the same location of the primary fixation, and the MCTR was sutured transsclerally using the same surgical technique. The conjunctiva was approximated to the limbus with interrupted 8-0 polyglactin 910 sutures. Finally, clear corneal incisions were secured to be watertight. Gentamicin (20 mg) was injected subconjunctivally at the conclusion of the surgery.
The early postoperative period was uneventful. At 3 and 6 months’ follow-up, best-corrected visual acuity was 20/32. Cystoid macular edema was identified and verified with posterior segment optical coherence tomography (OCT; RTVue XR 100, Optovue Inc, Fremont, CA) and was treated with topical nonsteroid anti-inflammatory drugs, oral carbonic anhydrase inhibitor, and periocular triamcinolone injection. No IOL tilt was observed during slit-lamp and anterior segment OCT examination.
Electron Microscopic and Spectroscopic Study of the New and Extracted 9-0 Polypropylene Sutures and New MCTRs
The explanted 9-0 loop polypropylene (MANI 1486L) sutures and new sutures of the same caliber and manufacturer were dehydrated, followed by critical point drying, and were mounted on metal stubs to be coated with aluminum (50 nm) using an electron beam evaporator (MEB 550S; Plassys, France). The samples were then analyzed with scanning electron microscopy (SEM; JEOL JSM 7001F, Tokyo, Japan) operated at voltages of 1–30 kV.
Elemental mapping was carried out by energy dispersive X-ray analyzer Bruker XFlash 6|30 (EDX) attached to a JEOL JSM 7001F operating at a voltage of 20 kV. The spectrograms were compared to packaged and never-used sutures.
Because the MCTR was not explanted, newly available MCTRs provided by different manufacturers (Reper-NN; Morcher GmbH, Stuttgart, Germany) were studied with SEM within the same parameters. To investigate the full profile of the fixating loop, it was suggested that the MCTRs be transected by the femtosecond laser (LensX; Alcon Inc, Fort Worth, TX). The three new MCTRs (one Morcher sample and two Reper-NN samples) were affixed to the flat hydrophobic surface with plasticine to prevent sample micromotions during femtosecond laser transection. The laser parameters were limited to single-line fragmentation, with a minimal length of 3.0 mm, energy of 8.0 μJ and tangential spot separation and layer separation of 6.0 μm. Sodium hyaluronate 1.0% was used to fill the laser interface after docking by carefully injecting it with the 23 G cannula while simultaneously observing the laser monitor to ensure the absence of air bubbles in proximity to the MCTR. The pattern of the laser cut was positioned in the plane of the theoretical suture position bisecting the fixation loop encompassing the distal area of the MCTR.
In the online OCT scan, no hyperreflectivity was observed corresponding to the MCTR location in the video, because the plane of the scan differed from the transection orientation, mostly because of the sample’s transparency. After confirming the transection parameters, femtosecond laser fragmentation was performed.
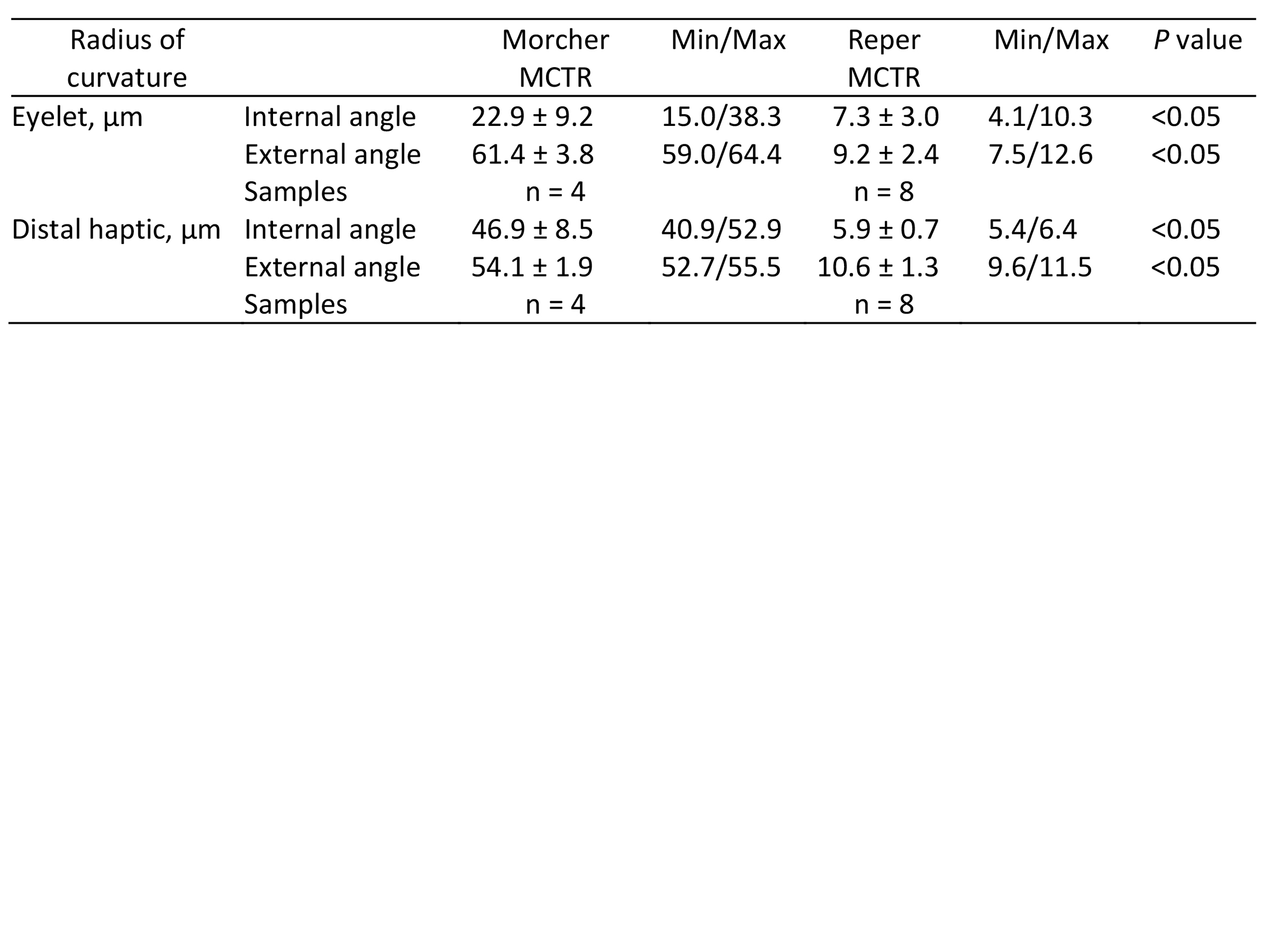
AutoCAD 2019 software (Autodesk, San Rafael, CA) was used to calculate the radius of curvature of the MCTRs’ cross-sectional profiles (3-4 angles in each sample); this was converted to micrometers according to the SEM scale bar. To avoid measurement error due to possible irregularities of the surface that cannot be defined in two-dimensional photographs, multiple measurements were performed from both distal sides of all fragments. The composite of 4 and 8 cross-sectional profiles of the fragments of the eyelet and 2 and 4 of the divided haptic were then evaluated in all samples (both Morcher and Reper MCTRs).
Statistical Analysis
StatPlus:Mac LE (AnalystSoft Inc, Vancouver, Canada) was used for statistical analysis. Normality of the data distribution was checked using the Shapiro-Wilk test. A P value of <0.05 was considered statistically significant. A paired t test was used to compare the radius of curvature parameters if mean differences between two unrelated measurements were of statistical significance.
Results Laboratory Study of the Polypropylene Sutures
The new polypropylene suture was of good quality, with no signs of biodegradation: the surface was smooth, no cracks were identified, and good symmetry was observed. Rare and minor production defects, consisting of longitudinal abrasion marks were noted (Figure 2A).
The SEM images showed that both parts of the suture that were extracted from the intrascleral tunnels (the distal ends of the suture) had undergone surface biodegradation. The increased roughness of the surface was identified through the multiple transversal cracks with deposits of debris, but no significant change in the diameter was seen (Figure 2B).
Carbon (C) can be observed in the spectrograms, because it is the main component of the adhesive tape used for sample fixation. Oxygen spikes resulted from metal oxides and/or from the water adsorbed on the surface of the sample or the chamber of the microscope. The method of EDX is otherwise insensitive to hydrogen. Given these confounders, quantitative estimates of the samples given below may be inaccurate, but they are minute enough to define qualitative consistency.
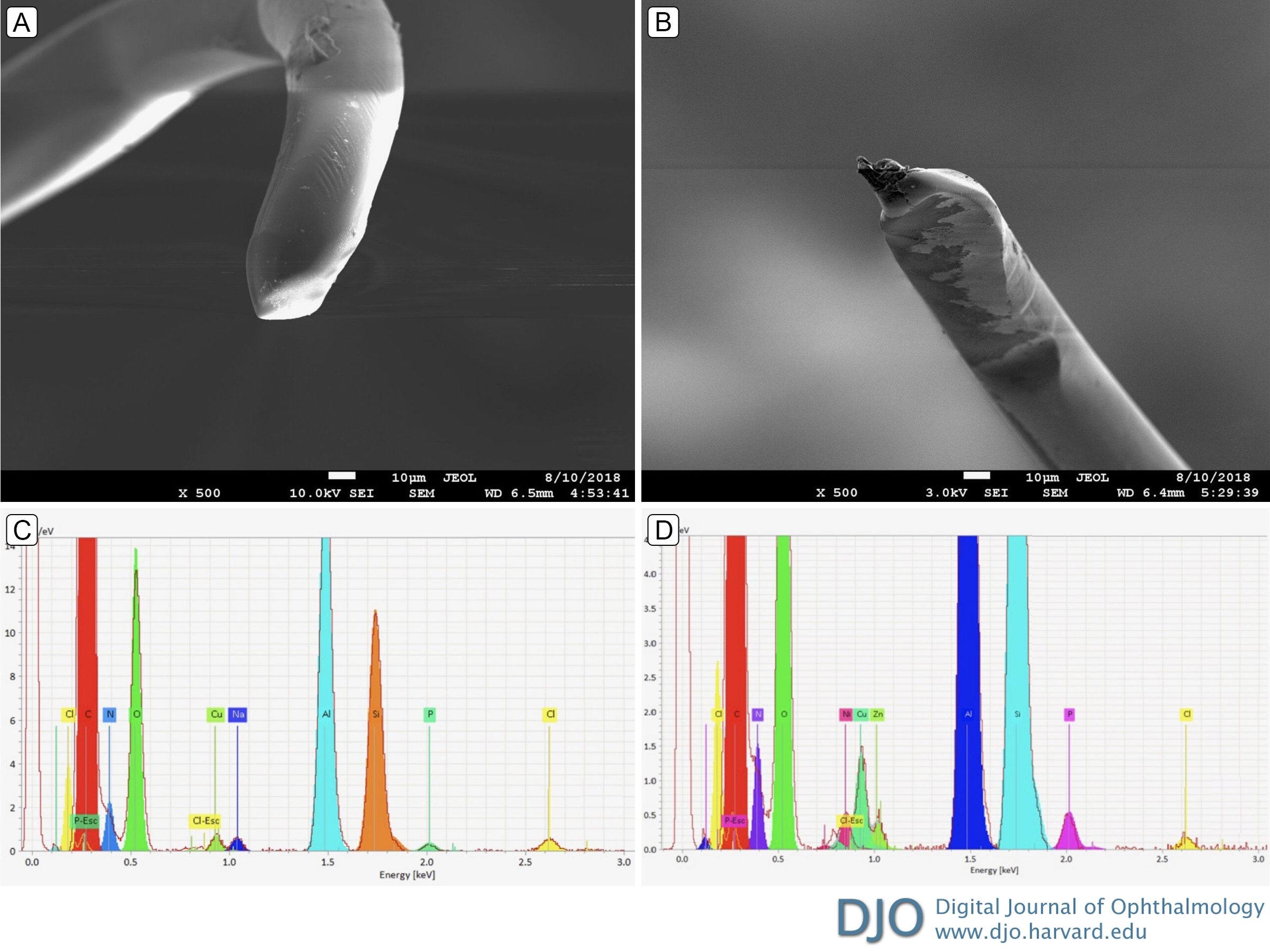
The elemental profile of the new control suture included spikes caused by the silicon (Si) substrate and the microscope chamber copper (Cu), zinc (Zn), nickel (Ni), and silicon wafer (Figure 1C). The EDX of the intrascleral parts of the explanted suture, however, showed significantly different elemental consistencies (Figure 2D; Table 1) from the proximal sections of the new suture, which were smooth and had no features of biodegradation. The ends of the explanted suture were asymmetrical, with gradual narrowing toward the apex. Concave flattening was observed in proximity to the apex with in situ laceration at the very end (Figure 3A-B). Although elemental changes were identified, they were less extensive compared with the intrascleral parts of the suture (Figure 3C-D; Table 1).
Laboratory Study of MCTRs
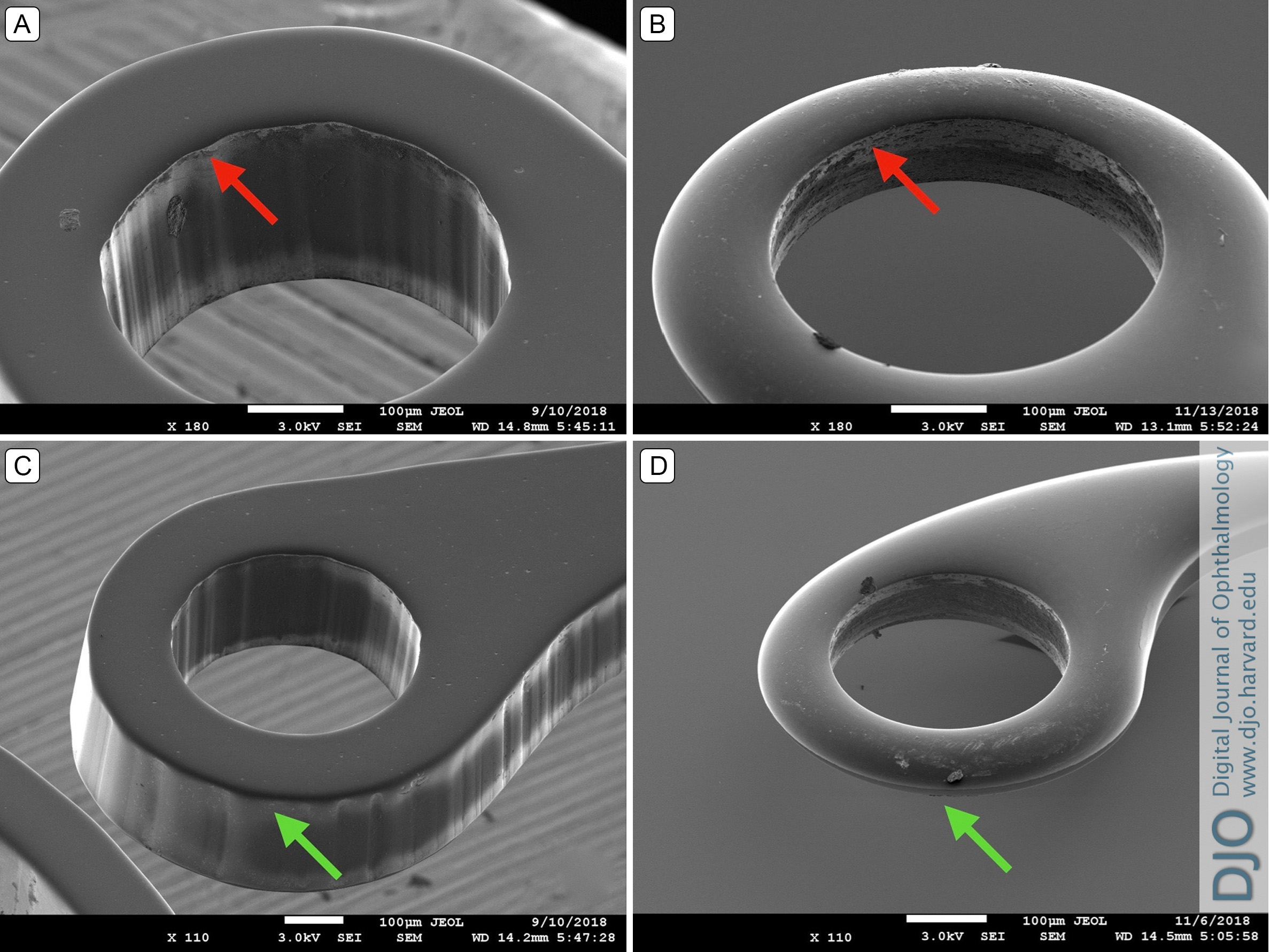
The SEM revealed the presence of sharp edges in both types of MCTRs (Figure 4); however, in cross-section, the radius of curvature of the two brands of MCTR edges differed significantly, with the Morcher MCTR looking smother (Figure 5D; Table 2). In addition to the haptic cross-section both the Reper-NN inner side (Figure 4A, 5B) and outer side (Figure 4C, 5B) of the fixation loop were sharper than the Morcher MCTR. However unlikely, although the outer side of the Morcher MCTR eyelet was smoother (Figure 4D), the inner side appeared to be sharp, but only at the eyelet (Figure 4B). The haptic of the Morcher MCTR was smooth on both sides (Figure 5D).
Table 1
Qualitative elemental profile of new and different parts of the explanted suture by energy dispersive X-ray analysis: main elements
Table 2
The radius of curvature of the cross-section Malyugin-modified capsular tension ring (MCTR) provides: Morcher versus Reper
Figure 1
Slit-lamp photographs of subluxated transscleral sutured capsular bag–intraocular lens (IOL)–Malyugin-modified capsular tension ring (MCTR) complex in the inferior temporal direction 5 years after implantation. A, Direct gaze, showing the edge of the IOL optic bisecting the pupil. B, View of the 9-0 polypropylene Z-suture in the inferior temporal quadrant. C, View of the 9-0 polypropylene Z-suture in the upper nasal quadrant.
Figure 2
Scanning electron microscopy (original magnification ×1500) and EDX-spectroscopy of the new (A,C) and the explanted (B,D) polypropylene 9-0 suture material. A, The suture structure is symmetrical with smooth surface and no features of biodegradation. B, Circumferential wrinkling of the suture is observed, but the wrinkles pass around the suture at right angles to its axis; the fracture is slightly oblique. C, The elemental profile of the new control suture included artifactual spikes caused by the microscope chamber and silicon substrate (silicon, copper, zinc, nickel). D, The elemental profile of the control suture included sodium, sulfur, phosphorus, potassium, and calcium.
Figure 3
Scanning electron microscopy (original magnification ×500) and EDX-spectroscopy of the distal parts of the explanted 9-0 polypropylene suture material. A, The suture structure is asymmetric, with gradual narrowing toward the apex; the surface is smooth, without features of biodegradation. B, Concave flattening is observed in proximity to the apex with in situ laceration at the very end of the suture breakage. C, The elemental profiles of the suture ends are similar, except for the absence of natrium at one end of the suture. D, The expected natrium could be hidden by the peak of zinc.
Figure 4
Scanning electron microscopy of various MCTRs manufacturers (Reper-NN, Russia; Morcher GmbH, Germany) at ×180 and ×110 magnification from various observation points. A, The relatively sharp edge of the inner side of the Reper-NN MCTR eyelet (red arrow). B, The relatively sharp edge of the inner side of the Morcher MCTR eyelet (red arrow). C, The overall view of the MCTR (Reper-NN, Russia) fixation eyelet constituting the presence of the relatively sharp edge of the outer side (green arrow). D, The overall view of the MCTR (Morcher GmBH, Germany) fixation eyelet showing the presence of a relatively sharp edge at its inner side (green arrow).
Figure 5
The AutoCAD report of the SEM photographs (original magnification ×300). The radius of curvature of the cross-section Morcher and Reper MCTRs profiles are shown in micrometers (converted according to the present scale bar of 10 µm). The internal and external parts are highlighted in red and green, respectively. A-B, The fragment of the eyelet Morcher MCTR and Reper MCTR, respectively. C-D, The fragment of the haptic Morcher MCTR and Reper MCTR, respectively.
Video 1
Primary surgery. Cataract surgery was performed with consequent implantation of the MCTR (Reper-NN, Nyzhny Novgorod, Russia) transsclerally sutured with 9-0 polypropylene using a cow-hitch and Z-suture technique.
Video 2
Repeat surgery. Refixation surgery was performed by transsclerally suturing MCTR haptic with the cow-hitch technique using the 9-0 polypropelene in the two opposite directions.
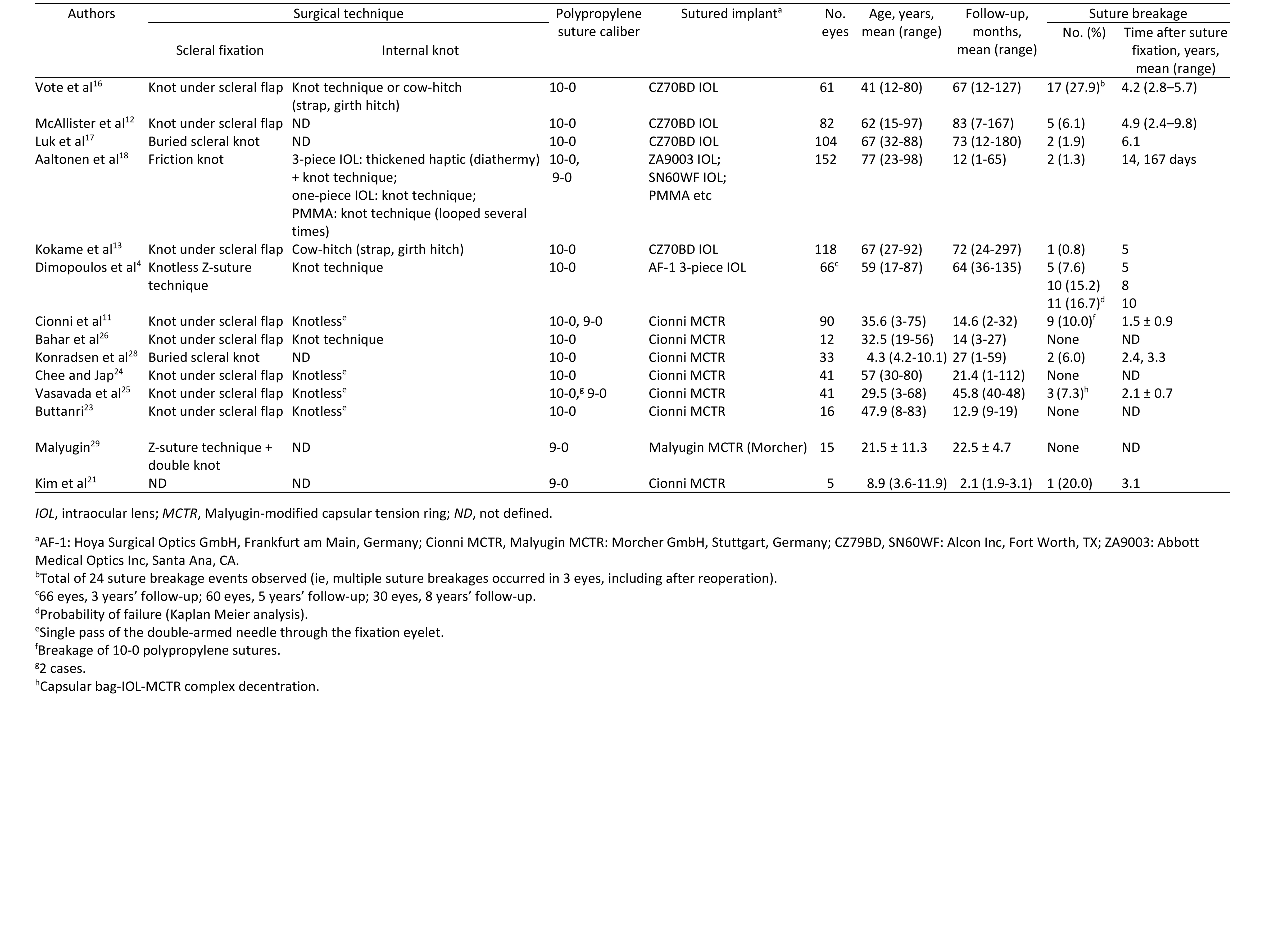
The most common indications for MCTR implantation with transscleral suture fixation are Marfan syndrome (40.3%), idiopathic zonular insufficiency (27.2%), and previous trauma (22.8%).(10) The weighted average of indicated zonular insufficiency for deciding to implant the MCTR has been reported as 173°. The described procedure allows for improved vision in up to 75.4% of cases, with the restoration of capsular bag centration and minimized IOL tilt.(10) Despite the favorable functional and anatomical outcomes, one of the most common postoperative complications is suture breakage, requiring subsequent repeated fixation surgery (Table 3).
Scleral suture fixation is widely used for repair of subluxed intraocular implants (IOL, artificial iris diaphragm, MTCR). However, the risk of early- and long-term dislocation of the fixated intraocular implant is relatively high and may lead to a dramatic visual decline.(11-13) The etiology of most cases that fail to provide significant improvement remains undefined. Potential causes of sutured implant dislocation are suture biodegradation,(1) idiopathic suture breakage,(11-13) chronic abrasion, erosion of the suture through the tissue,(14) knot untying,(15) knot slippage, and iatrogenic damage to the suture. One reported risk factor for suture breakage is young age, with the assumption that this association is due to increased saccadic motions and more active lifestyle, causing continuous microtrauma to the suture.(16) Postoperative fibrotic response leads to contractile centripetal forces followed by anterior phimosis or general capsular contraction syndrome increasing tension on sutures, especially in microspherophakia, further predisposing to suture breakage in the long term.
The rate of suture breakage in scleral-fixated IOLs is reported to range from 0.8% to 28% at ≥12 months.(4,12,13,16-18) Rebreakage after repair occurs in 5% of patients, who then require multiple surgeries.(16) Aaltonen et al reported 2 cases (1.3%) of suture breakage in a large cohort after 14 and 167 days.(18) The authors identified intraoperative damage of the suture as the main reason for early failure of suture fixation in these cases. Cionni et al identified a 10-0 polypropylene suture breakage rate of up to 10% when sutured to the MCTR in 1.5 ± 0.9 years after surgery.(11) These experiences have led to the use of larger caliber polypropylene (9-0 or 8-0),(19,20) CV-8 Gore-Tex (off label), or other fixation techniques. Our study reveals the cause of 9-0 polypropylene suture breakage with MCTR fixation. A previous case of 9-0 polypropylene suture breakage was reported by Kim et al.(21)
Polypropylene suture, though widely accepted in ophthalmology, is a synthetic nonabsorbable polymer monofilament whose biodegradation is reportedly higher in more highly vascularized tissues, such as the limbus and sclera, coinciding with our findings.(1) Our case identified the transition zone between the biodegraded suture and the intact section to be where the suture entered the intraocular aqueous filled compartment. Given that 10-0 polypropylene shows no degradation after 13 years when used for iris-suture fixation,(22) we conclude that the substrate of aqueous humor significantly reduces cellular antigenic response to the suture material by constant aqueous flow. This suture position likely isolates the material from the factors that induce biodegradation. The suture located in the scleral tunnel underwent only superficial changes (Figure 2B), which did not change suture diameter, confirmed by comparison with the manufacturer’s new Polypropylene suture (Figure 2A). We believe that the evidence shows that years of chronic abrasion by the sharp edge of the MCTR eyelet is the cause of breakage and fixation loss. Our microelemental profile findings exclude the etiology of biodegradation due to chemical suture lysis in our case as the explanted polypropylene suture was similar to a new suture sample. We cannot exclude the possibility of intraoperative damage having been a triggering factor as the MCTR was placed and fixed prior to phacoemulsification. It is recommended that all steps of lens removal be performed with the capsule hooks in place if there are weak or missing zonules and consequently place and suture the MCTR once the bag is empty. This puts far less stress on the suture and sclera, preventing intraoperative suture damage.
Mechanical degradation of suture material can be caused by compression, tension, and/or shearing forces. Occasionally, these abiotic factors act in synergy with or may initiate or accelerate the biodegradation process. This may be why young patients and eye rubbers have an increased risk of degraded suture integrity. Our patient reported no ocular or head trauma, suggesting that the superior zonular defect might have been due to gradual loss of zonular integrity, likely exacerbated by surgical intervention and primary zonular pathology. Redistribution of zonular tension could have contributed to degradation of suture integrity.
Suturing technique as well as suture caliber can play a significant role in the timing of MCTR fixation failure. Fixation to the MCTR eyelet with a knotless technique, though common, is accompanied by constant micromotions that can cause continuous abrasion.(11,23-25) The presence of a knot in the eyelet fixation significantly increases the size of the eyelet-suture knot complex(26) and may induce pigment dispersion by close contact with the iris. By comparison, the cow-hitch (strap hitch), a knotless technique, reduces the overall volume of the suture-eyelet complex while lending stability by reducing torque. Regardless of technique, however, the sharp edge of the MCTR eyelet will influence suture destruction after primary or refixation surgery. It remains unknown which part of the radius of curvature within the eyelet is in contact with the suture and causes its destruction—the primary reason for IOL dislocation in our case.
The internal knot should be stable and of minimal spatial volume. The suture technique of the distal part of the suture should be chosen according to the same principles. The Z-suture technique was used in our case for both primary and repeat surgery.(4,27)
Future studies should compare the in vitro abrasion resistance of various sutures to the edges of intraocular device edges and eyelets. Data on the endurance of suture integrity may result in a recommendation to manufacturers to soften edges of the intraocular implants intended to come in contact with various suture materials.
Meeting Presentation
Presented at the Annual Meeting of the American Society of Cataract and Refractive Surgery Annual Meeting, San Diego, California, May 3-7, 2019.
Support
This work was performed using equipment of MIPT Shared Facilities Center and with financial support from the Ministry of Education and Science of the Russian Federation (grant RFMEFI59417X0014).
Financial Disclosures
Boris Malyugin has a financial interest in Malyugin-modified CTR and the Malyugin ring pupil expansion device.
1. Price MO, Price FW, Werner L, Berlie C, Mamalis N. Late dislocation of scleral-sutured posterior chamber intraocular lenses. J Cataract Refract Surg 2005;31:1320-6.
2. Parekh P, Green WR, Stark WJ, Akpek EK. Subluxation of suture-fixated posterior chamber intraocular lenses. Ophthalmology 2007;114:232-7.
3. Byrd JM, Young MP, Liu W, et al. Long-term outcomes for pediatric patients having transscleral fixation of the capsular bag with intraocular lens for ectopia lentis. J Cataract Refract Surg 2018;44:603-9.
4. Dimopoulos S, Dimopoulos V, Blumenstock G, et al. Long-term outcome of scleral-fixated posterior chamber intraocular lens implantation with the knotless Z-suture technique. J Cataract Refract Surg 2018;44:182-5.
5. Hanemoto T, Ideta H, Kawasaki T. Dislocated intraocular lens fixation using intraocular cowhitch knot. Am J Ophthalmol 2001;131:265-7.
6. Hanemoto T, Ideta H, Kawasaki T. Luxated intraocular lens fixation using intravitreal cow hitch (girth) knot. Ophthalmology 2002;109:1118-22.
7. Nakashizuka H, Shimada H, Iwasaki Y, Matsumoto Y, Sato Y. Pars plana suture fixation for intraocular lenses dislocated into the vitreous cavity using a closed-eye cow-hitch technique. J Cataract Refract Surg 2004;30:302-6.
8. Seki M, Yamamoto S, Abe H, Fukuchi T. Modified ab externo method for introducing 2 polypropylene loops for scleral suture fixation of intraocular lenses. J Cataract Refract Surg 2013;39:1291-6.
9. Chen SX, Lee LR, Sii F, Rowley A. Modified cow-hitch suture fixation of transscleral sutured posterior chamber intraocular lenses: long-term safety and efficacy. J Cataract Refract Surg 2008;34:452-8.
10. Li B, Wang Y, Malvankar-Mehta MS, Hutnik CM. Surgical indications, outcomes, and complications with the use of a modified capsular tension ring during cataract surgery. J Cataract Refract Surg 2016;42:1642-8.
11. Cionni RJ, Osher RH, Marques DM, Marques FF, Snyder ME, Shapiro S. Modified capsular tension ring for patients with congenital loss of zonular support. J Cataract Refract Surg 2003;29:1668-73.
12. Mcallister AS, Hirst LW. Visual outcomes and complications of scleral-fixated posterior chamber intraocular lenses. J Cataract Refract Surg 2011;37:1263-9.
13. Kokame GT, Yanagihara RT, Shantha JG, Kaneko KN. Long-term outcome of pars plana vitrectomy and sutured scleral-fixated posterior chamber intraocular lens implantation or repositioning. Am J Ophthalmol. 2018;189:10-16.
14. Solomon K, Gussler JR, Gussler C, Meter WSV. Incidence and management of complications of transsclerally sutured posterior chamber lenses. J Cataract Refract Surg 1993;19:488-93.
15. Price FW, Whitson WE. Visual results of suture-fixated posterior chamber lenses during penetrating keratoplasty. Ophthalmology 1989;96:1234-40.
16. Vote BJ, Tranos P, Bunce C, Charteris DG, Cruz LD. Long-term outcome of combined pars plana vitrectomy and scleral fixated sutured posterior chamber intraocular lens implantation. Am J Ophthalmol 2006;141:308-12.
17. Luk ASW, Young AL, Cheng LL. Long-term outcome of scleral-fixated intraocular lens implantation. Br J Ophthalmol 2013;97:1308-11.
18. Aaltonen P, Oskala P, Immonen I. Outcomes of intraocular lens scleral fixation with the friction knot technique. Acta Ophthalmol 2019:97:e506-13.
19. John T, Tighe S, Hashem O, Sheha H. New use of 8-0 polypropylene suture for four-point scleral fixation of secondary intraocular lenses. J Cataract Refract Surg 2018;44:1421-5.
20. Shin YU, Seong M, Cho HY, Kang MH. Novel technique to overcome the nonavailability of a long needle 9-0 polypropylene suture for sutured scleral fixation of the posterior chamber intraocular lens using a single fisherman’s knot. J Ophthalmol 2017;1-4.
21. Kim EJ, Berg JP, Weikert MP, et al. Scleral-fixated capsular tension rings and segments for ectopia lentis in children. Am J Ophthalmol 2014;158:899-904.
22. Coleman M. Report of a 10-0 polypropylene suture that did not undergo biodegradation after 13 years in the eye. Digit J Ophthalmol 2016;22:66-7.
23. Buttanri IB, Sevim MS, Esen D, Acar BT, Serin D, Acar S. Modified capsular tension ring implantation in eyes with traumatic cataract and loss of zonular support. J Cataract Refract Surg 2012;38:431-6.
24. Chee S-P, Jap A. Management of traumatic severely subluxated cataracts. Am J Ophthalmol 2011;151:866-71.
25. Vasavada AR, Praveen MR, Vasavada VA, et al. Cionni ring and in-the-bag intraocular lens implantation for subluxated lenses: a prospective case series. Am J Ophthalmol 2012;153:1144-53.
26. Bahar I, Kaiserman I, Rootman D. Cionni endocapsular ring implantation in Marfans syndrome. Br J Ophthalmol 2007;91:1477-80.
27. Szurman P, Petermeier K, Aisenbrey S, Spitzer MS, Jaissle GB. Z-suture: a new knotless technique for transscleral suture fixation of intraocular implants. Br J Ophthalmol 2010;94:167-9.
28. Konradsen T, Kugelberg M, Zetterström C. Visual outcomes and complications in surgery for ectopia lentis in children. J Cataract Refract Surg. 2007;33:819-24.
29. Malyugin B. The results of cataract surgery in patients with Marfan’s syndrome with the new CTR. Zdrav Vestn Suppl 2012:61-6.
 Welcome, please sign in
Welcome, please sign in