|
|
 |
|
|
|
|
|
Iris melanin pigment as a masquerade of Gram-positive cocci after penetrating ocular trauma
Digital Journal of Ophthalmology
2018
Volume 24, Number 4
October 18, 2018
DOI: 10.5693/djo.02.2018.07.002
|
Printer Friendly
Download PDF |
|
|

Wenlan Zhang, MD | Duke University Eye Center, Durham, North Carolina Alan Proia, MD, PhD | Duke University Eye Center, Durham, North Carolina; Department of Pathology, Duke University, Durham, North Carolina Sumit Sharma, MD | Cleveland Clinic, Cole Eye Institute, Cleveland, Ohio David Fleischman, MD, MS, FACS | Department of Ophthalmology, University of North Carolina, Chapel Hill, North Carolina
|
|
|
| Abstract | | We describe a case of penetrating eye injury that resulted in a post-injury day 1 hypopyon, leading to concern for endophthalmitis and phacoanaphylaxis. A Gram stain prepared by the clinical microbiology laboratory was interpreted as Gram-positive cocci (GPC). However, when cultures returned negative, further investigation with microbiology and pathology found that what was thought to be GPC was actually iris melanin pigment. Although endophthalmitis following ocular trauma remains an important diagnosis to consider, this microbiologic masquerade of iris melanin pigment as GPC should be considered in cases where Gram stain is positive yet cultures return negative. | | | Case Report | A 13-year-old white boy presented at Duke University Eye Center following a penetrating thumbtack injury to the left eye. At initial presentation, the patient endorsed pain and decreased vision. Review of systems was otherwise unremarkable. On examination, visual acuity was 20/70, and there was a 1.5 mm, full-thickness, paracentral corneal laceration that was self-sealing and Seidel negative. There was disruption of the lens through the iris, with a loose lens capsule and focal opacification of the lens. Given an intact globe and no evidence of an intraocular foreign body, he was discharged with an eye shield, topical antibiotics and steroids. At follow-up in the morning, still <24 hours from injury, he returned with new eye pain, and the visual acuity had decreased to 20/200. Intraocular pressure was 15 mm Hg, the conjunctiva was hyperemic, and the wound was briskly Seidel positive. There was a new 1 mm hypopyon in the anterior chamber, with significant cellular reaction and flare. The decreased visual acuity was consistent with rapid opacification of the lens. The iris was now notable for many large, engorged blood vessels. Even though the timeline was rather early for phacoanaphylaxis,(1) the apparent isolation of this robust inflammatory reaction to the anterior chamber raised suspicion that the patient had developed phacoanaphylaxis, but infection could not be ruled out.
The Retina Service was consulted and, following an ultrasound that showed no vitreous opacities or retinal thickening, they also felt that the course and clinical examination was atypical for endophthalmitis. However, to rule out both phacoanaphylaxis and possible endophthalmitis, the decision was made to obtain aqueous sampling for cultures and Gram stain and to proceed with primary lensectomy without implantation of an intraocular lens, primary repair of corneal laceration, and injection of intravitreal vancomycin and ceftazidime, which the patient tolerated well.
On the first postoperative day, visual acuity with a +9.00 lens was 20/50, the hypopyon had resolved, and the anterior chamber revealed significant pigment, with only minimal cellular reaction. Dilated fundus examination revealed clear vitreous and no retinal involvement. Despite clinical evidence arguing against endophthalmitis, the Gram stain returned with rare Gram-positive cocci (GPC). The patient was treated subsequently with topical broad-spectrum antibiotics and carefully monitored as post-traumatic endophthalmitis, but his condition improved rapidly and further intervention was not needed. Given the positive Gram stain, it was surprising that cultures eventually returned negative.
With the unusual circumstance of having a positive Gram stain with negative cultures, the case was discussed in detail with the microbiology team. The microbiology lab, on review of the Gram stain slides, noted slight differences in the sizes of the putative GPC. On further investigation and with input from the Ocular Pathology Department, it was discovered that what was thought to be GPC was iris melanin pigment. On examination 1 year after the procedure, the patient had visual acuity of 20/20 with an aphakic rigid gas permeable lens. | |

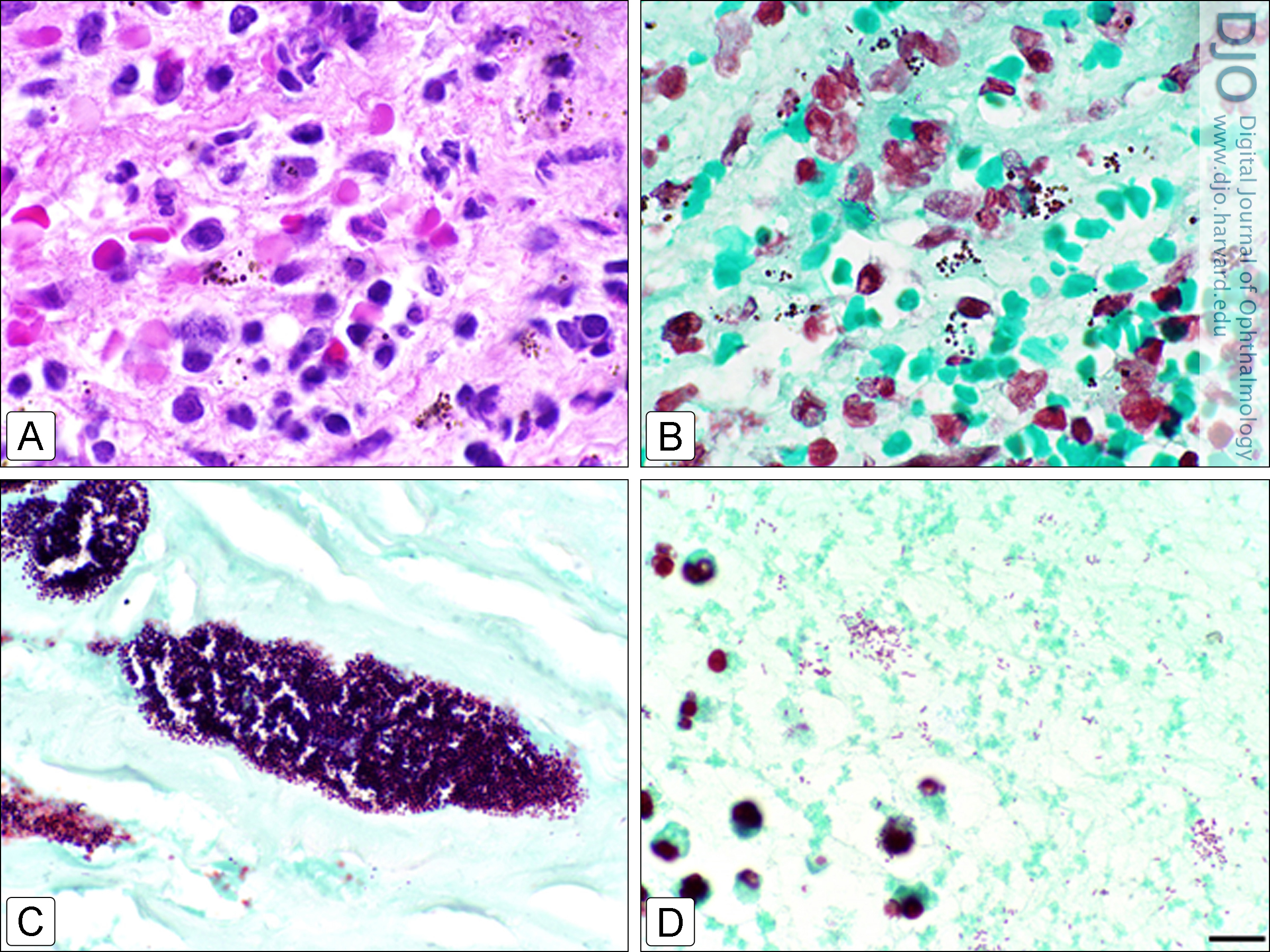
Figure 1
Iris pigment granules are shown within inflamed corneal stroma of a patient with a corneal perforation. A, Brown-Brenn modified Gram stain. B-D, hematoxylin and eosin stain. All images are at the same magnification (bar = 10 µm). The images are not from the patient reported in this case but from our own histopathologic collection. These images are representative of the similarities between iris melanin pigment and Gram-positive cocci that resulted in the microbiologic masquerade reported in the current case. In contrast to the iris melanin in A and B, a case of a failed penetrating keratoplasty graft due to infection with Staphylococcus aureus (C) and a sample from an eye with endophthalmitis due to Serratia marcescens (D), a Gram-negative bacillus, underscores the similarities in appearance.
|
|
| Discussion | Penetrating open-globe injuries are common in male children, with literature reports of lens involvement occurring in 24.2%-73% of open-globe injury eyes and endophthalmitis occurring in 4.9%-54.2% of injured eyes.(1) Standard guidelines were followed in the current case, with closure of primary wounds within 24 hours of injury. Despite closure within this timeline, our patient remained at greater risk for posttraumatic endophthalmitis because of involvement of the lens capsule.(1) Staphylococcus and streptococcus (GPC) are commonly isolated organisms in cases of endophthalmitis, with the latter being the most common causative organism in pediatric post-traumatic endophthalmitis.(1-3) In cases of clinically suspected endophthalmitis, cultures of the vitreous, aqueous, cornea, or other tissues may be beneficial in establishing the diagnosis.(4) As demonstrated in our case, whereas Gram stains are used as an initial fast screen to distinguish bacterial species, they have poor sensitivity compared to culture results.(5) In a large retrospective series spanning the period 1997-2004 at a single, tertiary-care center, bacterial culture results from patients with infectious keratitis were reviewed. A total of 453 patients were identified with bacterial infectious keratitis; cultures were positive in 307 cases (68%). Of the 334 cases for which Gram stain results were available and compared to culture results, Gram stain sensitivity was 18%, specificity was 94%, positive predictive value was 85%, and negative predictive value was 36%.(5) Other studies found that culture negativity of microbial keratitis was not uncommon. Sensitivity of cultures in identifying culprit organisms have been reported to fall within 60%-70%.(6-8)
Risk of culture negativity has been associated with longer use of topical antimicrobial medication prior to specimen acquisition.(9) Lack of a sample of traumatic lens material and the absence of positive cultures does not provide for a histopathologic diagnosis. However, even with a culture’s limitations, culture negativity, results of our institution’s Retina Service consultation, and the patient’s clinical course were consistent with a diagnosis of phacoanaphylactic uveitis.
Post-traumatic endophthalmitis is a devastating and common complication of globe injury; phacoanaphylaxis, or lens-induced uveitis, however, is a less common entity that requires very different management. Clinical assessment remains key in distinguishing these entities, but laboratory testing aids in the diagnosis and treatment planning. Zonal granulomatous inflammation is a characteristic histopathologic finding of this entity, although it is of questionable utility in most clinical settings. A large clinicopathologic review found that the earliest reported phacoanaphylaxis presentation in the literature was 2 days following injury.(10) Our case presented 1 day following injury.
Iris pigment granules resembling GPC and Gram-negative bacteria are a well-known phenomenon of masquerade in ocular pathology and ocular microbiology.(3,4,11,12) However, there are, to our knowledge, no reported clinical cases, series, or studies reporting this confounding appearance, its consequences, and its management. Since Gram stains are relied on for initial clinical assessment of infection status and potential culprit organisms and may change medical management, it is important for eye-care providers to know that pigment granules from the iris or retinal pigment epithelium may resemble GPC and Gram-negative bacteria, similar to the representative images detailed in Figure 1A-D. Durand et al noted that the two entities may be distinguished by the fact that pigment granules are more refractile than bacteria.(3,4) The refractility can be enhanced by closing, at least partially, the condenser aperture diaphragm which increases contrast and thus refractility. Other features are also important. Melanosomes from the retinal pigment epithelium, particularly in its apical projections, are often elongated and therefore may resemble Gram-negative rods. Melanosomes are usually brown or golden in color, even with Gram staining, while GPC are a deep bluish-purple color. This difference may not be apparent until one has compared GPC to melanosomes in a Gram-stained specimen. Melanosomes tend to vary more in size and shape than clusters of bacteria. When evaluating a Gram-stained ophthalmic specimen, it is useful to search first for bacteria in areas that are free of pigmented cells. Clinically, the eye-care provider may perform an anterior chamber paracentesis in a suspected case of phacoanaphylaxis, which may reveal polymorphonuclear leukocytes, histiocytes and plasma cells surrounding amorphous lens material.(13) It is recommended to review images and illustrations of ophthalmic infections in order to increase the clinician’s diagnostic acumen.(14)
Although clinical suspicion for infection must remain high given the devastating consequences of unrecognized infection and delayed treatment, this microbiologic masquerade should be considered in similar cases where Gram stain is positive, yet cultures return negative, particularly in cases that do not follow a clinical course consistent with endophthalmitis. It is important for the treating ophthalmology team to recognize the potential for confusion on Gram stain and pathology specimens between melanin pigment and bacteria.
Literature Search
PubMed (1970-present) was searched for English-language results on October 17, 2018, using the following terms: phacoanaphylaxis; phacoantigenic uveitis; iris pigment AND bacteria; iris pigment AND Gram positive; iris pigment AND Gram negative; iris pigment AND endophthalmitis. We found no case studies that reported a clinical example of iris pigment masquerading as endophthalmitis.
Financial Support
University of North Carolina, Department of Ophthalmology, Cleveland Clinic Foundation, Department of Ophthalmology, and Duke University Eye Center are recipients of unrestricted grants from Research to Prevent Blindness, Inc (New York, NY). | | | References | 1. Li X, Zarbin MA, Bhagat N. Pediatric open globe injury: a review of the literature. J Emerg Trauma Shock 2015;8:216-23.
2. Ahmed Y, Schimel AM, Pathengay A, Colyer MH, Flynn HW Jr. Endophthalmitis following open-globe injuries. Eye (Lond) 2012;26:212-17.
3. Durand ML. Endophthalmitis. Clin Microbiol Infect 2013;19:227-34.
4. Durand ML. Bacterial and fungal endophthalmitis. Clin Microbiol Rev 2017;30:597-613.
5. Yeh DL, Stinnett SS, Afshari NA. Analysis of bacterial cultures in infectious keratitis, 1997 to 2004. Am J Ophthalmol 2006;142:1066-8.
6. American Academy of Ophthalmology. Cornea/External Disease Panel, Preferred Practice Pattern Guidelines, Bacterial Keratitis. San Francisco, CA: American Academy of Ophthalmology, 2011.
7. Gopinathan U, Sharma S, Garg P, Rao GN. Review of epidemiological features, microbiological diagnosis and treatment outcome of microbial keratitis: experience of over a deacade. Indian J Ophthalmol 2009;57:273-9.
8. Basak SK, Basak S, Mohanta A, Bhowmick A. Epidemiological and microbiological diagnosis of suppurative keratitis in Gangetic West Bengal, eastern India. Indian J Ophthalmol 2005;53:17-22.
9. Bhadange Y, Das S, Kasav MK, Sahu SK1, Sharma S. Comparison of culture-negative and culture-positive microbial keratitis: cause of culture negativity, clinical features and final outcome. Br J Ophthalmol 2015;99:1498-1502.
10. Thach AB, Marak GE Jr, McLean IW, Green WR. Phacoanaphylactic endophthalmitis: a clinicopathologic review. Int Ophthalmol 1991;15:271-9.
11. Wilhelmus KR. Laboratory tests in the diagnosis of ocular infections. In: Tasman W, Jaeger EA, eds. Duane’s Foundations of Clinical Ophthalmology, vol 2. Philadelphia: JB Lippincott Company; 1994.
12. Okumoto M. Laboratory diagnosis of endophthalmitis. Int Ophthalmolo Clin 1987;27:89-94.
13. Hochman M, Sugino IK, Lesko C, Friedman AH, Zarbin MA. Diagnosis of phacoanaphylactic endophthalmitis by fine needle aspiration biopsy. Ophthalmic Surg Lasers 1999;30:152-4.
14. Stagner AM, Jakobiec FA, Eagle RC, Charles NC. Infections of the eye and its adnexa. In: Kradin RL, ed. Diagnostic Pathology of Infectious Disease. 2nd ed. Philadelphia: Elsevier; 2018:648-85. | |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in