|
|
 |
|
|
|
|
|
Report of a 10-0 polypropylene suture that did not undergo biodegradation after 13 years in the eye
Digital Journal of Ophthalmology
2016
Volume 22, Number 3
August 25, 2016
|
Printer Friendly
Download PDF |
|
|

Michael Coleman, MD | Cornea Division, Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, Maryland Uri Soiberman, MD | Cornea Division, Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, Maryland Walter J. Stark, MD | Cornea Division, Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, Maryland
|
|
|
| Abstract | | We report the case of a 70-year-old man who underwent surgery to fixate a subluxated intraocular lens. A 10-0 polypropylene suture that had been placed 13 years prior was retrieved intraoperatively and subsequently imaged using electron microscopy. The suture showed no clinically significant signs of biodegradation. | | | Introduction | | Aphakia without capsular support may be treated with iris-sutured intraocular lenses (IOLs) utilizing 10-0 polypropylene sutures; however, many surgeons believe that the long-term stability of this type of suture is questionable and that it undergoes biodegradation.(1) This notion leads to the use of larger caliber 9-0 polypropylene, CV-8 Gore-Tex, or other fixation techniques, such as intrascleral haptic fixation or scleral-glued IOLs.(2,3) This report demonstrates the long-term stability of 10-0 polypropylene sutures. | | | Case Report | A 70-year-old myopic man presented at Wilmer Eye Institute with blurred vision. On examination, his best-corrected visual acuity was 20/20 with an aphakic correction of +7.00 +0.75 ×90. Anterior segment examination revealed that a previously placed IOL in the right eye was dislocated. The patient’s history was remarkable for a rhegmatogenous retinal detachment managed initially with a scleral buckle procedure and later with a pars plana vitrectomy. The same eye subsequently developed IOL subluxation that required iris suture fixation with 10-0 polypropylene sutures using the modified McCannel technique nearly 13 years before presentation. The fixation sutures had been placed on the haptics (not through any eyelets).
The patient underwent surgery to correct the subluxated IOL. During surgery, the original 10-0 polypropylene sutures placed on the haptics were found to be intact. The dislocated IOL was brought to pupillary capture and resutured to the iris. At the last follow-up visit, the patient’s best-corrected visual acuity was 20/25 with a ?1.75 +1.00 ×180 refractive correction.
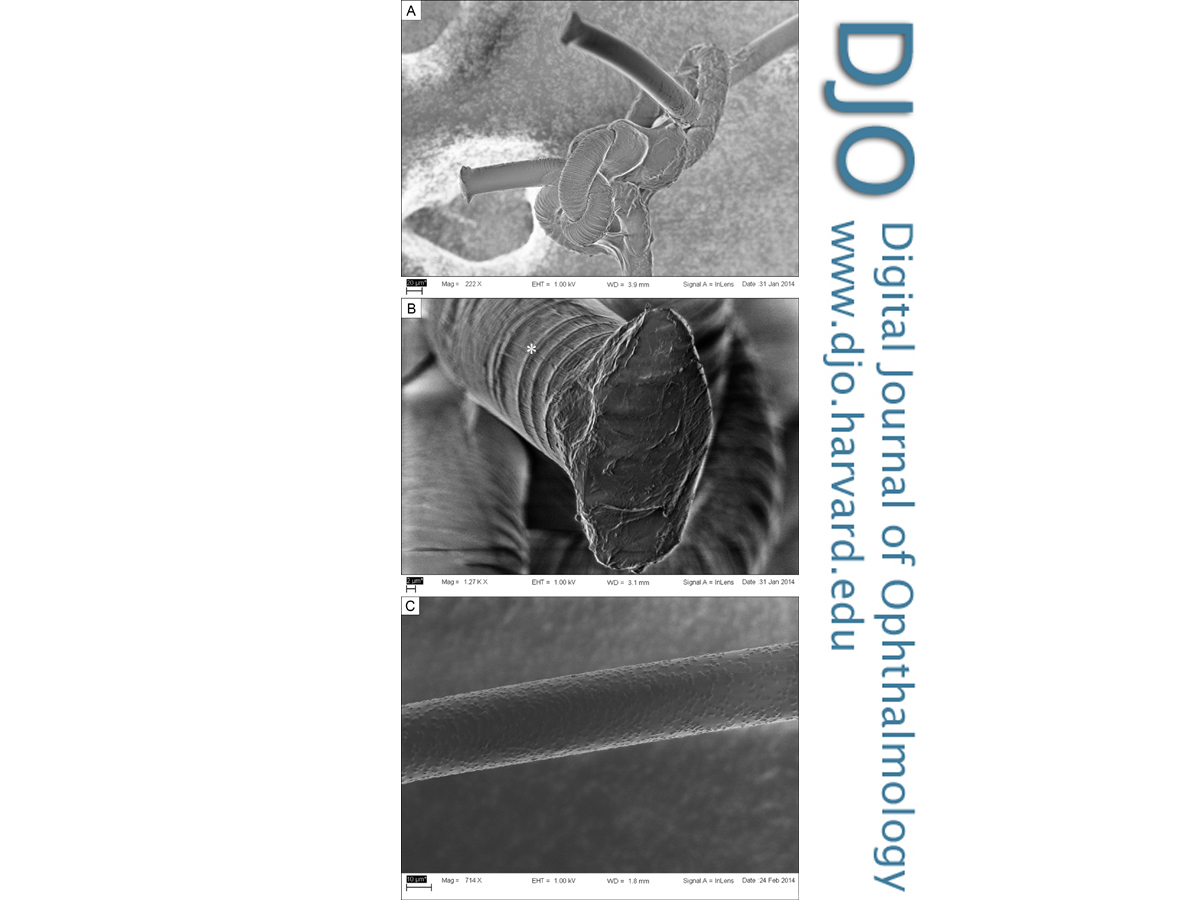
Prior to iris-suture fixation, the old sutures were cut and sent for examination with scanning electron microscopy. Figure 1A-B demonstrate that the knot is intact and that although transverse cracking is present, it is superficial and therefore does not significantly reduce the circumference of the suture or its tensile strength. Figure 1C demonstrates a control suture – here, no transverse cracking is visible. | |

Figure 1
Electron microscopy images of a 10-0 polypropylene suture retrieved from the right eye of a patient. A, 13-year-old suture with intact knot. B, Cut edge with very superficial transverse clefting (asterisk). C, Control suture (new).
|
|
| Discussion | Our group previously reported the case of an 11.5-year-old 10-0 polypropylene suture retrieved from an eye with a recurrent subluxation of an iris sutured IOL.(4) That report concluded that this type of suture does not undergo significant biodegradation, but that the sharp edge of the eyelets of the IOL slowly cut through the suture. Price et al, utilizing light microscopy techniques to examine sutures from eyes with dislocated 10-0 polypropylene, sclerally sutured IOLs, showed that suture remnants displayed transverse clefting, which reduced the tensile strength of the suture.(5) In that report, the oldest retrieved suture was approximately 14 years, and 4 of 5 IOLs had eyelets used for fixation. We believe that suture placement through the eyelets accounts for recurrent subluxation in at least 4 of the 5 IOLs described by Price et al. The fifth eye had chronic iritis; in that case inflammation may have led to accelerated suture degradation.
The present case demonstrates that the 10-0 polypropylene sutures exhibited some superficial cracking over time; however, there was no significant reduction in suture diameter; thus the suture’s tensile strength was not compromised. Therefore, the dislocation was probably the result of suture erosion through the iris tissue. This finding, together with our previous report that showed that the suture was cut by the sharp edges of the eyelets, suggests that suture biodegradation does not play a major role in the recurrent subluxations of sutured IOLs. If an IOL with an eyelet is used in these cases, the suture should be tied onto the haptic and not placed through the eyelet.
Financial Support
This research was supported by the Andreas C. Dracopoulos Fund. | | | References | 1. Buckley EG. Hanging by a thread: the long-term efficacy and safety of transscleral sutured intraocular lenses in children (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc 2007;105:294-311.
2. Prakash G, Jacob S, Ashok Kumar D, Narsimhan S, Agarwal A, Agarwal A. Femtosecond-assisted keratoplasty with fibrin glue assisted sutureless posterior chamber lens implantation: new triple procedure. J Cataract Refract Surg 2009;35:973-9.
3. Scharioth GB, Prasad S, Georgalas I, Tataru C, Pavlidis M. Intermediate results of sutureless intrascleral posterior chamber intraocular lens fixation. J Cataract Refract Surg 2010;36:254-9.
4. Parekh P, Green WR, Stark WJ, Akpek EK. Subluxation of suture-fixated posterior chamber intraocular lenses a clinicopathologic study. Ophthalmology 2007;114:232-7.
5. Price MO, Price FW Jr, Werner L, Berlie C, Mamalis N. Late dislocation of scleral-sutured posterior chamber intraocular lenses. J Cataract Refract Surg 2005;31:1320-6. | |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in