|
|
 |
|
|
|
|
|
Anterior chamber cholesterolosis in a patient with retinoblastoma
Digital Journal of Ophthalmology
2016
Volume 22, Number 1
March 31, 2016
DOI: 10.5693/djo.02.2015.10.002
|
Printer Friendly
Download PDF |
|
|

Bryan K. Hong, MD | Retina Service, Wills Eye Hospital, Philadelphia, Pennsylvania Emil Anthony T. Say, MD | Vision Center, Children’s Hospital Los Angeles, Los Angeles, California Patricia Chévez-Barrios, MD | Department of Pathology, The Methodist Hospital, Baylor College of Medicine, Houston, Texas; Ocular Oncology Service, Wills Eye Hospital, Philadelphia, Pennsylvania Thomas C. Lee, MD | Vision Center, Children’s Hospital Los Angeles, Los Angeles, California Jonathan W. Kim, MD | Vision Center, Children’s Hospital Los Angeles, Los Angeles, California
|
|
|
| Abstract | | Anterior chamber cholesterolosis is a rare phenomenon typically associated with non-neoplastic conditions such as hyphema or Coats disease; it has never been reported to be associated with intraocular malignancy. We report a case of anterior chamber cholesterolosis presenting in the setting of retinoblastoma and discuss clinical features relevant for its differentiation from Coats disease. | | | Case Report | A 2-year-old Hispanic girl presented at Children’s Hospital–Los Angeles for evaluation of left periocular edema discovered during an examination for a urinary tract infection. Past medical and family history were unremarkable. On examination, visual acuity was fix and follow in the right eye and poor fix and follow in the left eye. Magnetic resonance imaging (MRI) showed bilateral intraocular masses with signal characteristics consistent with retinoblastoma, with possible invasion of the left optic nerve. Lumbar puncture and metastatic work-up were negative.
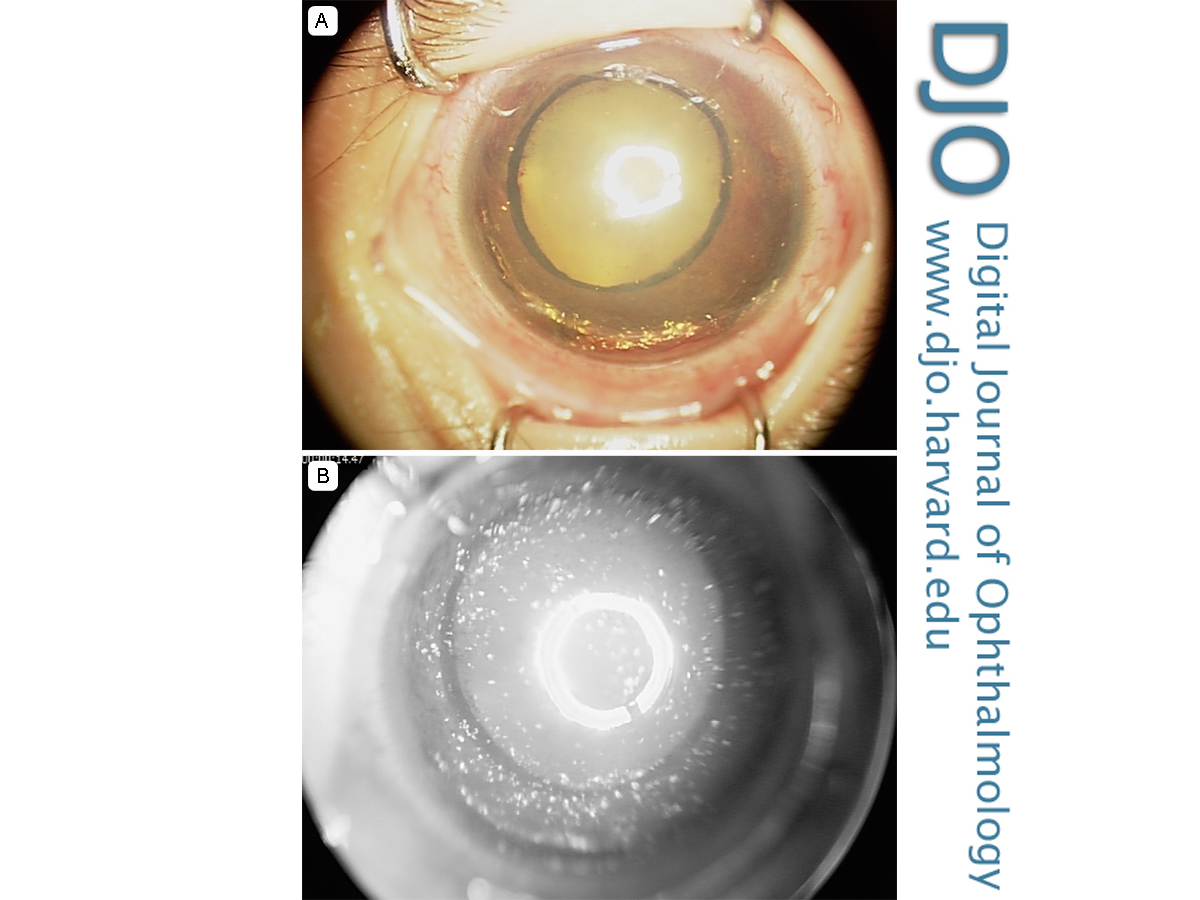
Examination under anesthesia showed a normal anterior segment in the right eye; however, the left eye showed xanthocoria, diffuse neovascularization of the iris, hyphema, fibrinous material on the anterior lens capsule, and yellow refractile crystals throughout the anterior chamber (Figure 1A). Intraocular pressures were normal in each eye. Fundus examination of the right eye revealed a single retinoblastoma in the temporal periphery with distant seeding along the inferior vitreous base. There was no fundus view in the left eye, but B-scan ultrasound showed a large intraocular mass, with calcification and vitreous opacities consistent with seeding and/or hemorrhage. There was autofluorescence of the anterior segment crystals. Fluorescein angiography showed autofluorescence of the anterior segment crystals as well as with diffuse leakage from iris neovascularization in the left eye and early hyperfluorescence of the peripheral tumor in the right eye, with dilated feeding vessels (Figure 1B).
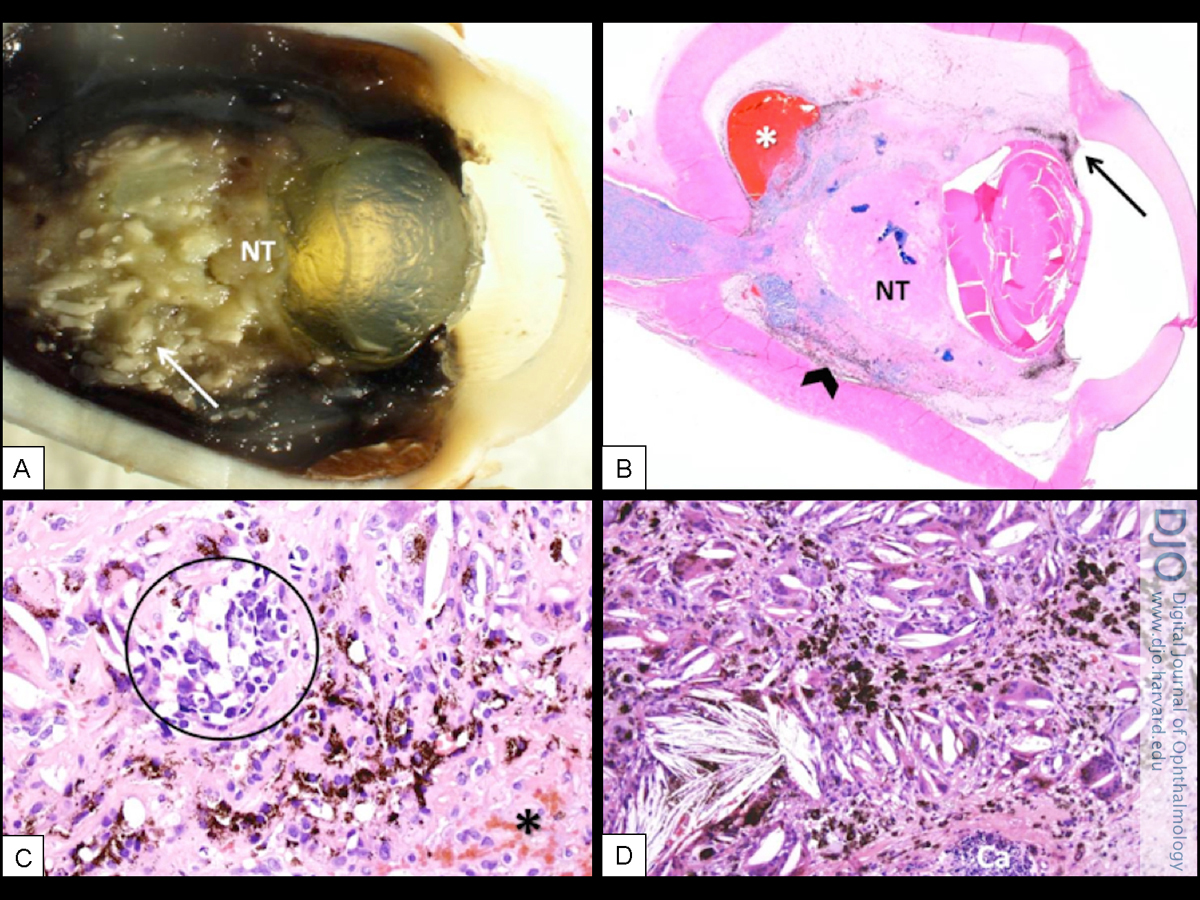
Clinical findings were consistent with bilateral retinoblastoma, International Classification of Retinoblastoma (ICRB) group D in the right eye and group E in the left eye. The first 2 of a planned 6 cycles of systemic chemotherapy with carboplatin, etoposide, and vincristine, were administered, followed by enucleation of the left eye 3 weeks after the second cycle. The enucleated eye showed numerous cholesterol crystals in the anterior chamber, vitreous, and subretinal space (Figure 2). A touch imprint under polarization showed the typical square crystals and the erythrocytes of the residual hemorrhage (Figure 2A-B). The crystals were seen to be surrounded by multinucleated giant cells (Figure 2C-D) in the anterior iris and in the subretinal space (Figure 3C,D). The majority of the tumor was necrotic or calcified; however, there were small residual foci of non-necrotic, noncalcified tumor in the subretinal space and in the head of the optic nerve (Figure 3A-C). | |
Figure 1
Figure 1. A, Clinical photograph of the left eye anterior segment showing xanthocoria, yellow refractile crystals, small hyphema, ectropion uvea, and neovascularization of the iris. B, Fluorescein angiogram of the left eye showing autofluorescent anterior segment crystals.
|
|

Figure 2
Histopathologic findings. A, Macroscopic photograph of the anterior segment with the crystals in the inferior angle (*) attached to the surface of the iris (I). The lens is slightly opaque (L). B, Polarization of a touch imprint of the crystals before processing shows the typical square shape. Notice the multiple crystals staked up. It also shows the erythrocytes of the residual hemorrhage on the surfaces of the crystals (arrow; Touch imprint under polarization, original magnification ×40). C, Histologic section of the peripheral iris (I) pigment dispersion secondary to previous necrosis. Note the thick neovascular and fibrous membrane on the surface of the iris containing the multinucleated giant cells with pigment and cholesterol clefts (arrow; hematoxylin and eosin [H&E], original magnification ×10). D, High-power view of the cholesterol granuloma in this membrane (H&E stain, origninal magnification ×40).
|
|

Figure 3
A, Macroscopic photograph of the cut surface of the eye with necrotic tumor (NT) and calcified tumor (arrow). B, Low-power view of the eye with areas of hemorrhage (*), necrotic tumor (NT), choroidal scar (arrow head) and anterior synechia of iris (arrow), with the crystals seen in 2C-D. Also note the square shape of the eye usually seen in atrophic eyes (H&E, original magnification: scan of slide). C, High-power view of the area near hemorrage (*), residual tumor (encircled), proliferation of retinal pigment epithelium (RPE; pigmented cells) and cholesterol crystals inside of multinucleated cells (H&E, original magnification ×20). D, Area of cholesterol granulomatous reaction near RPE (pigmented cells) and calcified tumor (Ca) (H&E, original magnification ×10).
|
|
| Discussion | Anterior chamber cholesterolosis has been observed after severe trauma, chronic inflammation, chronic retinal detachment, hyphema, vitreous hemorrhage, and Coats disease.(1-3) The cholesterol deposits are thought to be derived from the breakdown of intraocular hemorrhage.(2) To our knowledge, the present case is the first of a child with anterior chamber cholesterolosis in the setting of intraocular retinoblastoma. In our patient, hyphema, neovascularization of the iris, vitreous, and subretinal hemorrhage, and tumor necrosis were observed at presentation. One or more of these factors may have led to the formation of cholesterol crystals and cholesterol granulomata in the anterior chamber, but the exact mechanism is unclear. Our patient had a unique clinical presentation in her left eye: xanthocoria and anterior chamber cholesterolosis in the setting of advanced intraocular retinoblastoma. The performance of noninvasive imaging tests, such as MRI and ocular ultrasound, as well as a careful examination of the other eye, led to the correct diagnosis of retinoblastoma.
Literature Search
The authors conducted a MEDLINE search using the PubMed database (National Library of Medicine) through May 23, 2015. A combination of keywords were used, including the following terms: cholesterolosis, anterior chamber cholesterolosis, malignancy, and retinoblastoma. Words such as eye, ophthalmic, and intraocular were used and cross-referenced with various key words to retrieve the specific articles. The search was confined to articles in English or English abstracts. Inclusion and exclusion were based on relevance to the subject. | | | References | 1. Patel AK, Murphy M, Shields CL. Picture of the month: anterior chamber cholesterolosis in Coats disease. Arch Pediatr Adolesc Med 2011;165:1131-2.
2. Eagle RC Jr, Yanoff M. Cholesterolosis of the anterior chamber. Albrecht Von Graefes Arch Klin Exp Ophthalmol 1975;193:121-34.
3. Hemady R, Foster CS. Anterior chamber crystals following hyphema. Arch Ophthalmol 1990;108:14-5.
| |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in