|
|
 |
|
|
|
|
|
Iris-claw, retropupillary-fixated, aphakic intraocular lens implantation for traumatic aphakia following penetrating keratoplasty
Digital Journal of Ophthalmology
2015
Volume 21, Number 2
May 7, 2015
DOI: 10.5693/djo.02.2015.04.001
|
Printer Friendly
Download PDF |
|
|
 Anas A. Anbari, MD, PhD
Anas A. Anbari, MD, PhD | Department of Ophthalmology, Mouassat University Hospital, Damascus University, Damascus, Syria; Corneoplastic Unit and Eyebank, Queen Victoria Hospital, East Grinstead, United Kingdom; Ophthalmology Department, Eastbourne District General Hospital, Eastbourne, United Kingdom
|
|
|
| Abstract | | We report the correction of aphakia using an iris-claw, aphakic intraocular lens (IOL) fixated in a retropupillary location in a 17-year-old young man who suffered blunt trauma to his eye 5 months after penetrating keratoplasty (PKP). There were no intraoperative complications. At 21 months after implantation, the patient’s uncorrected distance visual acuity was 20/28; his corrected distance visual acuity was 20/22, with +0.50 −3.00 × 155. Intraocular pressure was normal, and endothelial cell count was 1798 cells/mm2. | | | Introduction | | The iris-claw intraocular lens (IOL) was originally developed for the treatment of aphakia in intracapsular cataract extraction surgery. Its indications have extended to include secondary IOL implantation to treat aphakia in cases with insufficient capsular support, including subluxated lens extraction,(1) traumatized eyes,(2) and keratoplasty.(3,4) We report our experience with retropupillary fixation of the iris-claw aphakic IOL (Ophtec BV, Groningen, The Netherlands) for the correction of aphakia following trauma, which resulted in subluxated cataractous lens, glaucoma, anterior synechiae, and vitreous prolapse in the left eye of a patient who had previously undergone left penetrating keratoplasty (PKP). | | | Case Report | A 17-year-old young man with a history of bilateral keratoconus presented at Mouassat University Hospital (Damascus University-Syria) having suffered blunt ocular trauma to his left eye 5 months after PKP in that eye. The trauma resulted in a dehisced PKP graft and subsequent open globe injury. The wound was repaired primarily and the same graft was sutured. Two months later the eye showed a subluxated cataract and anterior synechiae. At 7 months after the injury, following removal of the graft sutures and cessation of the associated topical corticosteroid treatment, the left eye showed raised intraocular pressure (IOP), which was unresponsive to medical treatment. A combined subluxated cataract extraction, trabeculectomy surgery, and anterior vitrectomy was performed to extract the subluxated cataract and to manage the elevated IOP and the anterior synechiae.
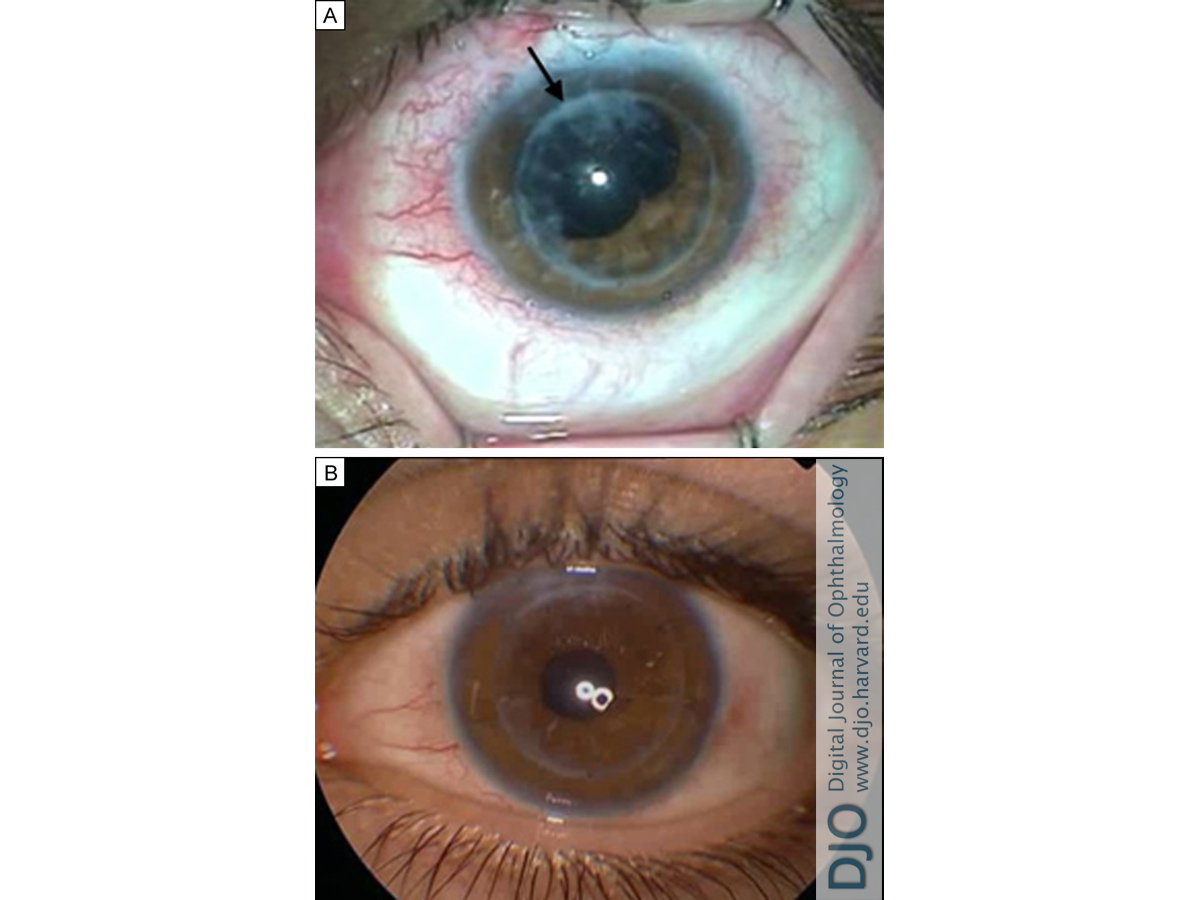
At 4 weeks’ after surgery the eye was aphakic with vitreous strand at the PKP incision and normal IOP without medications (Figure1A). Uncorrected distance visual acuity was 20/70 and best-corrected distance visual acuity was 20/25. On retinoscopy, refraction was +11.00 −4.00 ×160, with some irregular astigmatism. Keratometry readings were 42.00 ×160 and 47.50 ×070. The endothelial cell count was 2036 cells/mm2 (Topcon SP-2000P Non-Contact Specular Microscope, Topcon Corp, Tokyo, Japan). The anterior chamber depth was 3.32 mm.
An Artisan iris-claw aphakic IOL implantation fixated on the posterior iris and an anterior vitrectomy procedure was planned and performed after discussing the case with the patient and his parents. The patient’s glaucoma was controlled without medications from the prior surgery. A 5.0/8.5 mm +15.0 D Artisan iris-claw aphakic IOL was implanted in a reverse position, through a two-plane 5.5 mm posterior corneal (limbal) incision. We prefer a scleral tunnel; however, the presence of the bleb in this case did not afford sufficient room. The lens was fixated to the posterior surface of the iris, and interrupted sutures were used to control the postoperative astigmatism by selective postoperative suture removal.
At 5 months postoperatively, the IOP was normal, uncorrected distance visual acuity was 20/70 and best-corrected visual acuity was 20/22, with a refractive error correction of +3.25 −6.00 ×150 and keratometry readings of 43.50 ×150 and 48.50 × 060. A 10-0 polyester (Mersilene; Ethicon Inc, Somerville, NJ); compression suture was placed at axis 150° at the graft incision to treat the remaining refractive error.
At 21 months after Artisan aphakic IOL implantation (Figure 1B), uncorrected visual acuity was 20/28, and best-corrected visual acuity was 20/22 with a refraction of +0.50 −3.00 × 155. Keratometry readings were 45.25 × 155 and 48.25 × 065. IOP was normal. Endothelial cell count was 1798 cells/mm2. Trabeculectomy function was stable through the postoperative follow-up period of 12 months. | |

Figure 1
A, Preoperative view of the aphakic eye with normal IOP and vitreous wick at the penetrating keratoplasty incision (arrow) following subluxated cataract extraction, trabeculectomy, and anterior vitrectomy surgery (photography via operation microscope). B, Postoperative view showing Artisan iris-claw aphakic IOL retroiridis fixated implantation and anterior vitrectomy procedure (photography via anterior segment camera).
|
|
| Discussion | Artisan iris-claw aphakic IOL implantation has been used with good results as primary or secondary procedure to manage aphakia.(5) It has been used in subluxated lens extraction(1) and in traumatized eyes with insufficient capsular support for IOL implantation.(2) Implantation of iris-fixated IOLs with anterior iris fixation and with posterior iris fixation have been reported.(6)
In the present case, with insufficient capsular support, the refractive correction options were anterior chamber, angle-supported IOL, which was excluded because of possible complications with respect to endothelial cell loss and secondary glaucoma;(7,8) sclera-fixated posterior chamber IOL, which was also excluded because of possible complications with respect to suture cut, ciliary bogy hemorrhage, and cystoid macular edema;(9,10) and anterior, iris-fixated IOL, which was excluded on account of possible endothelial cell loss in general(11) and in particular compared to posterior iris-fixated IOL in PKP patients.(12)
Artisan iris-claw retropupillary fixated aphakic IOLs have been shown to be safe for aphakia in general(13,14) and in aphakia with keratoplasty.(3) An Artisan iris-claw retropupillary fixated aphakic IOL was implanted in our case after considering its good published results and the future possibility that the patient might have to undergo endothelial keratoplasty, which would be much more difficult in the presence of an anterior chamber IOL.(4,15,16) The retropupillary fixated IOL also does not prevent pupil dilation for posterior segment examination and treatment purposes.(14,17) In this case of traumatized PKP, implantation of iris-claw aphakic IOL with retropupillary fixation proved to be a feasible treatment with a good outcome, although the long-term outcome is unknown.
| | | References | 1. Aspiotis M, Asproudis I, Stefaniotou M, Gorezis S, Psilas K. Artisan aphakic intraocular lens implantation in cases of subluxated crystalline lenses due to Marfan syndrome. J Refract Surg 2006;22:99-101.
2. Riazi M, Moghimi S, Najmi Z, Ghaffari R. Secondary Artisan-Verysiseintraocular lens implantation for aphakic correction in post-traumatic vitrectomized eye. Eye 2008;22:1419-24.
3. Dighiero P, Guigou S, Mercie M, et al. Penetrating keratoplasty combined with posterior Artisan iris-fixated intraocular lens implantation. Acta Ophthalmol Scand 2006;84:197-200.
4. Karimian F, Sadoughi MM. Air-assisted Descemet-stripping automated endothelial keratoplasty with posterior chamber iris-fixation of aphakic iris-claw intraocular lens. J Cataract Refract Surg 2011;37:224-8
5. De Silva SR, Arun K, Anandan M, et al. Iris-claw intraocular lenses to correct aphakia in the absence of capsule support. J Cataract Refract Surg 2011;37:1667-72.
6. Wolter-Roessler M, Küchle M. Correction of aphakia with retroiridally fixated IOL. Klin Monatsbl Augenheilkd 2008;225:1041-4
7. Biro Z. Results and complications of secondary intraocular lens implantation. J Cataract Refract Surg 1993;19:64-7.
8. Ellerton CR, Rattigan SM, Chapman FM, et al. Secondary implantation of open-loop, flexible, anterior chamber intraocular lenses. J Cataract Refract Surg 1996;22:951-4.
9. Vote BJ, Tranos P, Bunce C, et al.Long-term outcome of combined pars plana vitrectomy and scleral fixated sutured posterior chamber intraocular lens implantation. Am J Ophthalmol. 2006;141:308-12.
10. Hara S, Borkenstein AF, Ehmer A, Auffarth GU. Retropupillary fixation of iris-claw intraocular lens versus transscleral suturing fixation for aphakic eyes without capsular support. J Refract Surg 2011;27:729-35.
11. Ing JJ, Ing HH, Nelson LR, et al. Ten-year postoperative results of penetrating keratoplasty. Ophthalmology 1998;105:1855-65.
12. Gicquel JJ, Guigou S, Bejjani RA, et al. Ultrasound biomicroscopy study of the Verisyse aphakic intraocular lens combined with penetrating keratoplasty in pseudophakic bullous keratopathy. J Cataract Refract Surg 2007;33:455-64.
13. Mohr A, Hengerer F, Eckardt C. Retropupillary fixation of the iris claw lens in aphakia: 1 year outcome of a new implantation technique. Ophthalmologe 2002;99:580-3.
14. Gonnermann J, Klamann MK, Maier AK, et al.Visual outcome and complications after posterior iris-claw aphakic intraocular lens implantation. J Cataract Refract Surg 2012;38:2139-43.
15. Beltz J, Busin M. Descemet stripping automated endothelial keratoplasty in a case with a posteriorly fixated iris-claw intraocular lens. Cornea 2012;31:96-7.
16. Anshu A, Price MO, Price FW Jr. Descemet’s stripping endothelial keratoplasty under failed penetrating keratoplasty: visual rehabilitation and graft survival rate. Ophthalmology 2011;118:2155-60.
17. Anbari A, Lake DB. Posteriorly enclavated iris claw intraocular lens for aphakia: long-term corneal endothelial safety study. Eur J Ophthalmol 2015;25:208-13. | |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in