Dan Z. Reinstein, MD, MA(Cantab), FRCSC, DABO, FRCOphth, FEBO | London Vision Clinic, London, United Kingdom; Department of Ophthalmology, Columbia University Medical Center, New York; Centre Hospitalier National d’Ophtalmologie, Paris, France Zachary Dickeson | London Vision Clinic, London, United Kingdom Timothy J. Archer, MA(Oxon), DipCompSci(Cantab) | London Vision Clinic, London, United Kingdom Marine Gobbe, MST(Optom), PhD | London Vision Clinic, London, United Kingdom
Incomplete flaps are a relatively uncommon complication of laser-assisted in situ keratomileusis (LASIK) that occur when creation of the corneal flap is interrupted. Further complications can arise if a second flap is created that intersects the original flap interface, resulting in tissue slivers that can lead to more complications and poor visual outcomes. We report the case of a 56-year-old man who underwent LASIK in which an incomplete flap occurred after 45% completion using a mechanical microkeratome with a 160 µm head. The maximum depth achieved by this incomplete flap was measured by very high-frequency (VHF) digital ultrasound as 182 µm peripherally. Two months later, a second flap was created beneath the incomplete flap, at a depth of 190 µm. The resulting flap had a central thickness of 196 µm and a minimum clearance of 30 µm beneath the incomplete flap. This demonstrates a method for creating secondary flaps that may significantly reduce the risk of flap interface intersection.
In fall 2007 a 56-year-old presbyopic man presented at the London Vision Clinic, London, to be assessed for laser-assisted in situ keratomileusis (LASIK). On examination, his manifest refraction was +1.00 −0.50 ×150 (20/16) in the right eye and +0.75 −0.25 ×48 (20/16) in the left eye with presbyopia. Preoperative corneal topography was considered normal in both eyes (Atlas 995; Carl Zeiss Meditec, Jena, Germany). Central corneal thickness was 606 μm in the right eye and 616 μm in the left eye (Corneo-Gauge Plus; Sonogage Inc, Cleveland, OH). White-to-white diameter was 12.0 mm in each eye (Orbscan II; Bausch & Lomb, Salt Lake City, UT). Vertical sinusoidal grid contrast sensitivity was normal (CSV-1000; VectorVision, Greenville, OH). Dilated fundus examination and biomicroscopic slit-lamp examination were unremarkable.
Primary Treatment
The treatment plan entailed bilateral LASIK, to be performed by one of the authors (DZR) using the Hansatome zero compression microkeratome (Bausch & Lomb, Salt Lake City, UT) with a 160 μm head and a 9.5 mm suction ring and the MEL80 excimer laser (Carl Zeiss Meditec, Jena, Germany). The nondominant right eye was to be treated with a target of −1.50 D for near vision and the dominant left eye with a target of plano for distance vision using the Laser Blended Vision module of the CRS-Master.(1) The nondominant right eye was treated first, but continued noncompliance and “squeezing” by the patient during the Hansatome flap creation resulted in a suction loss occurring after approximately 45% completion of the cut (see Video 1). The suction ring and microkeratome head were removed without incident. The partial flap was lifted and examined and found to be whole before being replaced; no ablation was performed. The left eye was not treated.
On postoperative day 1 the manifest refraction for the right eye was +1.25 −0.25 ×150 (20/16−2). The refraction remained stable at all visits from before surgery to 2 months after surgery (Table 1). At 1 month after surgery corneal curvature was only slightly elevated in a small area above the incomplete flap compared to preoperative corneal topography (Figure 1); overall the topography appeared normal. The maximum thickness of the incomplete flap was 162 µm (Visante OCT; Carl Zeiss Meditec, Jena, Germany), and contrast sensitivity was normal and unchanged.
Secondary Treatment
The thickness profile of the partial flap in the right eye across the central 10 mm diameter of the cornea was measured 2 months after surgery with the Artemis VHF digital ultrasound scanner (ArcScan Inc, Morrison, CO), which can measure flap thickness with a repeatability of 1.68 µm centrally and 3-4 µm paracentrally (Figure 2).(2) The thickness of the majority of the partial flap was between 120 μm and 150 μm. There was a localized region near the inferotemporal edge of the flap where the flap was much thicker, with a maximum thickness of 182 µm (Figure 3). In addition, the epithelial thickness profile revealed a >1 mm wide, linear zone of thinned epithelium across the scan diameter (Figure 3). The orientation and location of this zone was coincident with the limit of microkeratome cut across the cornea.
Following the original treatment, the VisuMax femtosecond laser (Carl Zeiss Meditec, Jena, Germany) had been installed at our clinic. Availability of the VisuMax made possible a follow-up procedure in this case to create a second flap with a precise flap depth. (The Hansatome microkeratome has a relatively less precise flap thickness reproducibility and is limited by the availability of only two head sizes, 160 μm or 180 μm.) The principal risk when creating a second flap is that the new interface could intersect the partial flap interface and result in tissue slivers.(3,4) To avoid interface crossover and tissue slivers a second flap must be created below the partial flap but still remain within the limits of residual stromal bed tissue. In our patient, the central corneal pachymetry was 601 μm and the refraction was low hyperopia, and it was determined that there was ample tissue available to make a second cut under the original half flap. Creating a second flap below rather than above the original flap was considered the safest option because this would avoid the risk of crossover with the epithelium. The reported flap thickness standard deviation with the VisuMax femtosecond laser is 7.9 μm.(5) Theoretically, to minimize the risk of a second flap crossing the interface of an existing flap, the thickness of the second flap should be two standard deviations below the existing flap. In the present case, one standard deviation was considered ample added depth, and the flap was planned with a thickness of 190 μm (182 μm + 8 µm), allowing for a wide margin under the majority of the incomplete flap. The inferotemporal edge of the flap was the only location felt to be at risk of interface crossover and would require special care when dissecting and lifting the new flap. Nevertheless, tissue slivers in this inferotemporal region would likely not have resulted in a visually significant complication. The potential error in the flap thickness measurement, with the paracentral repeatability of 3-4 µm, must also be taken into account. However, as above, because the thicker area of the flap was localized near the flap edge, it was decided not to add further bias to the flap thickness to avoid creating an excessively thick flap. This process is described in detail in Video 1.
The recut procedure was performed later the same day, after the Artemis scans had been analyzed and the flap thickness had been selected. Treatment was performed by one of the authors (DZR) using the VisuMax femtosecond laser and the MEL80 excimer laser. The flap was programed using an M-sized treatment pack to be 190 µm thick, 8.50 mm in diameter, with a superior hinge and a 105° side cut. Creation of a new flap interface beneath the original incomplete flap was completed successfully. Dissection and lifting of the VisuMax flap proceeded without incident, and no tissue slivers were found. Ablation with the MEL80 was performed according to the original treatment plan, with the nondominant right eye target as −1.50 D for near vision and the left eye target as plano for distance vision using the Laser Blended Vision module of the CRS-Master.(1) Treatment of the left eye was successful and uneventful.
At 1 day postoperatively, spherical equivalent refractions were −2.25 D in the right eye and −0.25 D in the left eye. Uncorrected binocular visual acuity at distance was 20/12.5−2 and J2 at near. Slit-lamp examination confirmed the flaps were positioned well, with no tissue slivers or microfolds present.
At 3 months postoperatively, manifest refractions were −1.00 −1.00 × 160 (20/16) in the right eye and plano (20/12.5−1) in the left eye. Uncorrected binocular visual acuity was 20/12.5 at distance and J1 at near. Corneal topographies were normal for post-hyperopic LASIK, with no irregularities due to the incomplete flap (Figure 1). Artemis scans were performed on the right eye to assess the thickness achieved by the VisuMax flap (Figure 4). The Reinstein flap thickness, calculated as the postoperative stromal component of the flap added to the preoperative epithelium, had a central thickness of 196 μm (maximum, 255 µm; minimum, 188 µm). The stromal tissue below the half-flap interface and above the VisuMax flap interface was found to have a maximum thickness of 110 µm and a minimum thickness of 30 µm (Figure 3). Contrast sensitivity was within normal limits.
At 1 year postoperatively, manifest refractions remained stable and were measured as −0.75 −1.25 ×155 (20/12.5−1) in the right eye and −0.25 −0.25 ×20 (20/12.5−1) in the left eye. Binocular visual acuity was 20/12.5−1 at distance and J1 at near. Contrast sensitivity was within normal limits. The patient was satisfied with his vision and reported good vision at near, intermediate, and far distances.
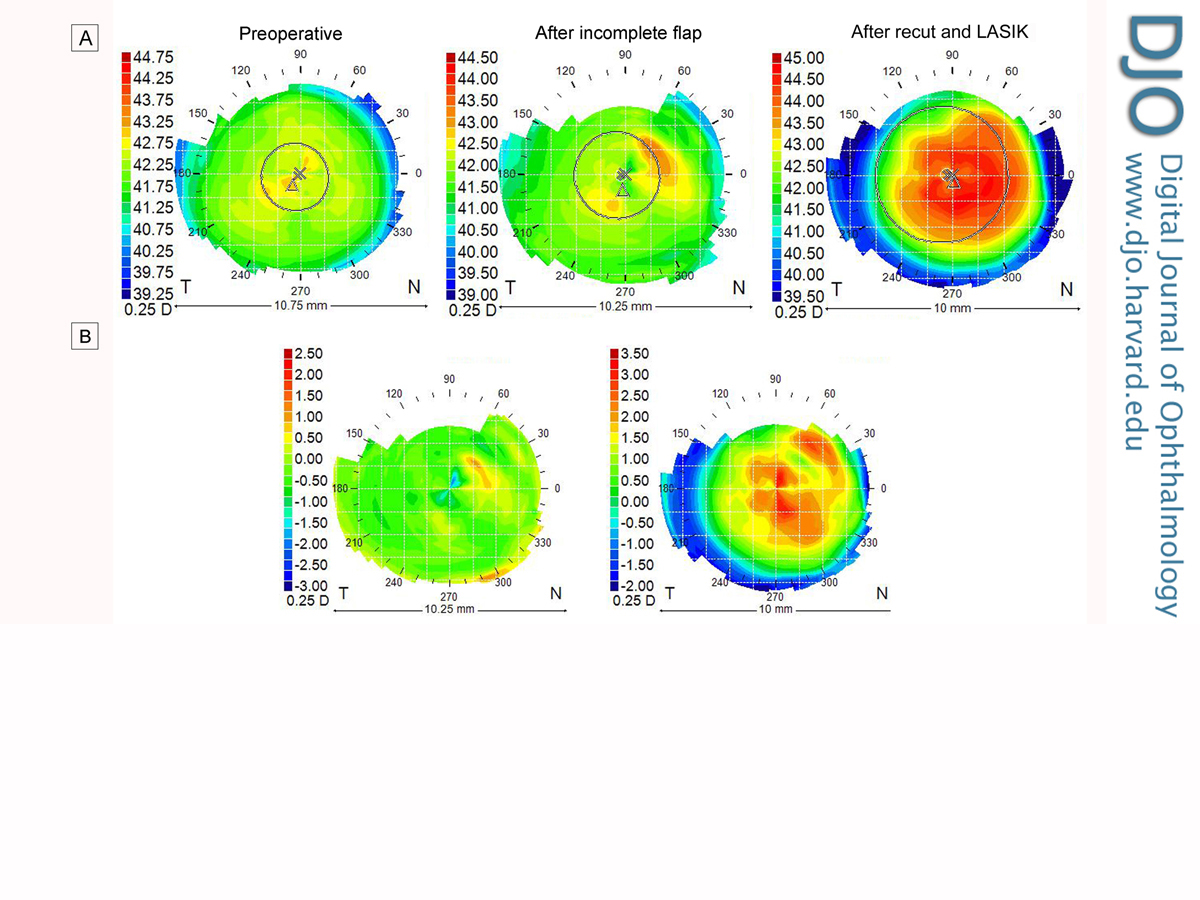
Figure 1
Atlas 995 axial curvature corneal topography (A) and axial curvature difference maps (B). Corneal topography remained largely unchanged as a result of the incomplete flap and showed typical central steepening as a result of hyperopic LASIK.
Figure 2
Nongeometrically corrected diagonal Artemis VHF digital ultrasound B-scan 2 months after the creation of an incomplete flap; the scan is oriented inferotemporal (left) to superonasal (right). The termination of the incomplete flap interface is clearly visible near the center of the image, confirming the extent of the partial flap. The maximum thickness of the incomplete flap was measured as 182 µm.
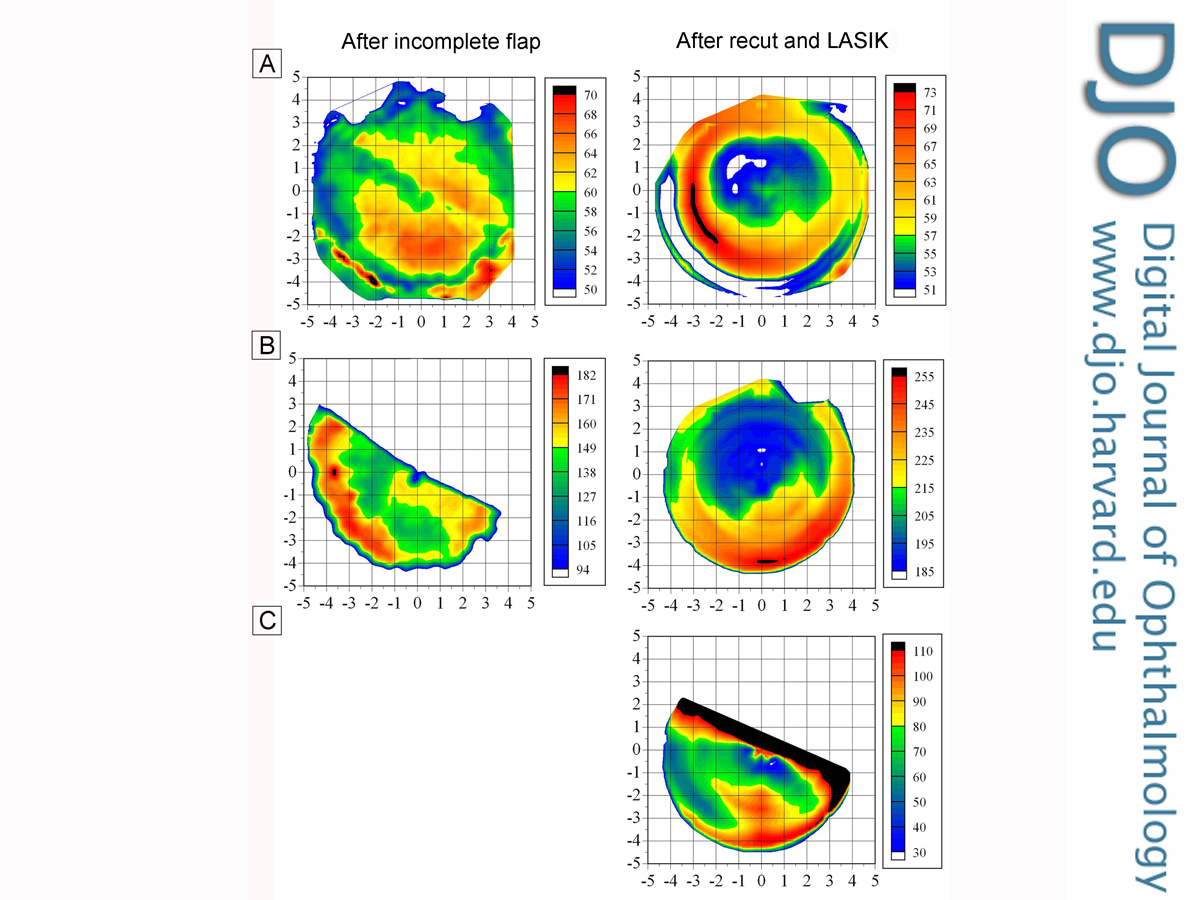
Figure 3
Artemis VHF digital ultrasound epithelial thickness maps (A), thickness of incomplete flap (B, left), secondary flap (B, right), and stromal thickness between incomplete and secondary flap interfaces (C). The epithelial thickness profile after the incomplete flap demonstrated a zone of thinning associated with the extent of the mechanical microkeratome cut. After the recut LASIK procedure, the epithelial thickness profile showed peripheral epithelial thickening, as expected after a hyperopic ablation. The flap thicknesses and the stromal thickness between them demonstrate the success of this treatment in avoiding interface crossover. Note that the difference in appearance between the two columns of maps is a result of the maps taken after the incomplete flap being produced using 18 B-scans and produced after the recut flap with 4 B-scans.
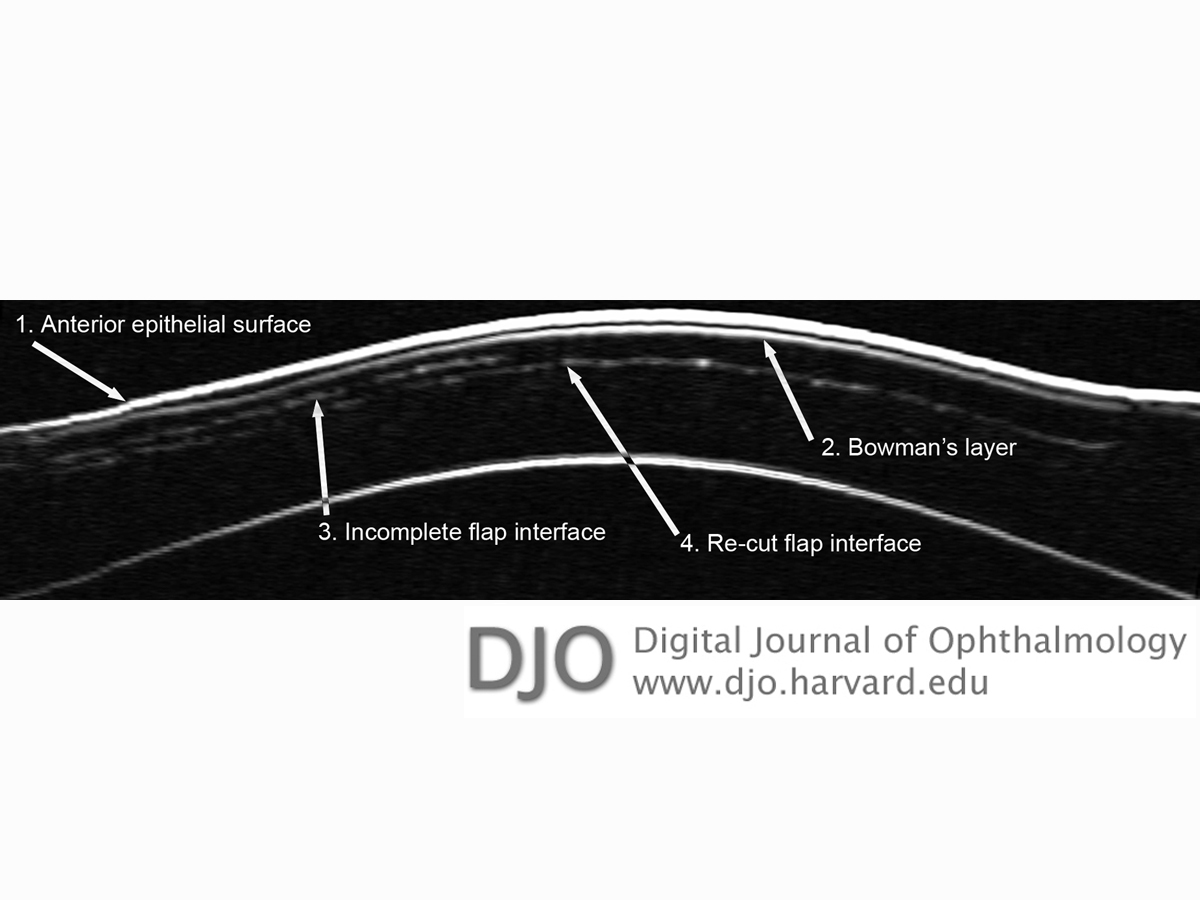
Figure 4
Nongeometrically corrected horizontal Artemis VHF digital ultrasound B-scan 3 months after the creation of a femtosecond flap and LASIK. Scan oriented horizontally from temporal (left) to nasal (right). The recut flap interface does not intersect the incomplete flap interface, and the space between the two interfaces was measured as 30 µm to 110 µm in thickness.
Table 1
Right eye manifest refractions and corrected distance visual acuity before and after the incomplete flap and after the secondary flap and ablation
Video 1
Summary of the entire case history including intraoperative footage from both procedures.
This case demonstrates a method for planning and recutting flaps using the Artemis VHF digital ultrasound arc-scanner and VisuMax femtosecond laser. The accurate measurement of an incomplete flap by optical coherence tomography or VHF digital ultrasound scanning is necessary to ascertain the actual flap thickness achieved.(5-7) A second flap can then be planned at a depth taking into account the reproducibility of both the femtosecond laser and the flap measurement device that will avoid crossover of the interfaces and the creation of tissue slivers. A femtosecond laser can then be used to create a second flap at a precisely planned depth to the nearest micron.
There are two other principal options for the management of a partial flap created with a mechanical microkeratome. The first is to switch to photorefractive keratectomy (PRK), which avoids any issue associated with the partial flap, but all the benefits of LASIK are lost. The second option is to recut a second flap using a mechanical microkeratome. However, due to the variability and nonuniformity of flap thickness with mechanical microkeratomes,(8-10) particularly with older models, a successful recut is difficult to achieve.
Without measurement and confirmation of the thicker-than-intended flap of 182 µm in the present case, the femtosecond laser recut may have been programmed as only 176 ¦Ìm (eg, 2 standard deviations above the intended flap depth of 160 µm). This would have resulted in a much higher likelihood of a crossover of the flap interfaces and the creation of tissue slivers. To avoid this scenario it may not always be possible to plan a suitably thick flap and remain within residual stromal tissue limits, so it is important to know the exact depth required.
In the present case, conservation of tissue was not an issue because of the high corneal pachymetry and low hyperopic refraction. In cases where conserving corneal tissue is a concern, the treatment accuracy of femtosecond lasers combined with an accurate flap thickness measurement may allow for the creation of a second flap between a previous flap interface and the epithelium. This is an option as long as the gap between the maximum epithelial thickness and the minimum thickness of the original flap is at least 4 flap thickness standard deviations, so that the second flap can be programmed with a thickness that is at least 2 standard deviations from both the epithelium and the original flap. For example, if the maximum epithelial thickness was 64 µm and the minimum thickness of the original flap was 106 ¦Ìm, a second flap could be safely programmed from 80 µm to 90 µm (80 – [2 × 8] = 64 ?m, 90 + [2 × 8] = 106 µm). This same technique can also be applied for retreatment after a previous LASIK in which a thick flap was created. In such patients, there may be insufficient residual stromal bed tissue required for the retreatment under the original flap. However, creating a second flap at a shallower depth is a viable alternative to retreating as PRK, provided there is enough space between the flap and the epithelium. Measurement of the epithelial thickness is particularly important in these cases because the epithelium thickens centrally after myopic ablation and paracentrally after hyperopic ablation.(11,12)
While rare, partial flaps are one of the most common complications related to mechanical microkeratome flap creation in LASIK.(13-15) For this reason it is important to have a good strategy for managing partial flaps that minimizes the increased incidence of complications related to recutting a second flap.(3,4,16) A direct measurement of the thickness profile of the partial flap is essential to assess the risks of creating a second flap, and using a femtosecond laser brings the advantages of good reproducibility and flap thickness uniformity as well as the ability to program the flap thickness to the nearest micron.
Financial disclosure
Dr. Reinstein has a proprietary interest in the Artemis technology (ArcScan Inc, Morrison, CO) and is the author of patents related to VHF digital ultrasound administered by the Cornell Center for Technology Enterprise and Commercialization (CCTEC), Ithaca, NY. Dr. Reinstein is a consultant for Carl Zeiss Meditec (Jena, Germany). The remaining authors have no proprietary or financial interest in the materials presented herein.
1. Reinstein DZ, Couch DG, Archer TJ. LASIK for Hyperopic astigmatism and presbyopia using micro-monovision with the Carl Zeiss Meditec MEL80 Platform. J Refract Surg 2009;25:37-58.
2. Reinstein DZ, Archer TJ, Gobbe M, et al. Repeatability of layered corneal pachymetry with the Artemis very high-frequency digital ultrasound arc-scanner. J Refract Surg 2010;26:646-59.
3. Tekwani NH, Chalita MR, Krueger RR. Secondary microkeratome-induced flap interference with the pathway of the primary flap. Opthalmology 2002;110:1379-83.
4. Peters NT, Iskander NG, Gimbel HV. Minimising the risk of recutting with a Hansatome over an existing Automated Corneal Shaper flap for hyperopic laser in situ keratomileusis enhancement. J Cataract Refract Surg 2001;27:1328-32.
5. Reinstein DZ, Archer TJ, Gobbe M, Johnson N. Accuracy and reproducibility of Artemis central flap thickness and visual outcomes of LASIK with the Carl Zeiss Meditec VisuMax femtosecond laser and MEL 80 excimer laser platforms. J Refract Surg 2010;26:107-19.
6. Salaroni CH, Li Y, Zhang X, et al. Repeatability of laser in situ keratomileusis flap thickness measurement by Fourier-domain optical coherence tomography. J Cataract Refract Surg 2011;37:649-54.
7. Reinstein DZ, Archer TJ, Gobbe M. Comparison of residual stromal bed thickness measurement among very high-frequency digital ultrasound, intraoperative handheld ultrasound, and optical coherence tomography. J Refract Surg 2012;28:42-7.
8. Reinstein DZ, Sutton HF, Srivannaboon S, Silverman RH, Archer TJ, Coleman DJ. Evaluating microkeratome efficacy by 3D corneal lamellar flap thickness accuracy and reproducibility using Artemis VHF digital ultrasound arc-scanning. J Refract Surg 2006;22:431-40.
9. Reinstein DZ, Archer TJ, Gobbe M. LASIK flap thickness profile and reproducibility of the standard vs zero compression Hansatome microkeratomes: three-dimensional display with Artemis VHF digital ultrasound. J Refract Surg 2011;27:417-26.
10. Yao P, Xu Y, Zhou X. Comparison of the predictability, uniformity and stability of a laser in situ keratomileusis corneal flap created with a VisuMax femtosecond laser or a Moria microkeratome. J Int Med Res 2011;39:748-58.
11. Reinstein DZ, Archer TJ, Gobbe M. Change in epithelial thickness profile 24 hours and longitudinally for 1 year after myopic LASIK: three-dimensional display with Artemis very high-frequency digital ultrasound. J Refract Surg 2012;28:195-201.
12. Reinstein DZ, Archer TJ, Gobbe M, Silverman RH, Coleman DJ. Epithelial thickness after hyperopic LASIK: three-dimensional display with Artemis very high-frequency digital ultrasound. J Refract Surg 2010;26:555-64.
13. Farah SG, Azar DT, Gurdal C, Wong J. Laser in situ keratomileusis: literature review of a developing technique. J Cataract Refract Surg 1998;24:989-1006.
14. Jacobs JM, Taravella MJ. Incidence of intraoperative flap complications in laser in situ keratomileusis. J Cataract Refract Surg 2002;28:23-8.
15. Moshirfar M, Gardiner JP, Schliesser JA, et al. Laser in situ keratomileusis flap complications using mechanical microkeratome versus femtosecond laser: retrospective comparison. J Cataract Refract Surg 2010;36:1925-33.
16. Tham VM, Maloney RK. Microkeratome complications of laser in situ Keratomileusis. Opthalmology 1999;107:920-4.
 Welcome, please sign in
Welcome, please sign in