|
|
 |
|
|
|
|
|
Artisan iris-fixated toric phakic intraocular lens for the correction of high astigmatism after deep anterior lamellar keratoplasty
Digital Journal of Ophthalmology
2013
Volume 19, Number 2
June 14, 2013
DOI: 10.5693/djo.02.2013.04.001
|
Printer Friendly
Download PDF |
|
|

Madonna Al-Dreihi, MD, MSc, FICO | Department of Ophthalmology, Mouassat University Hospital, Damascus University, Damascus, Syria Bachar Louka, MD, DIS | Department of Ophthalmology, Mouassat University Hospital, Damascus University, Damascus, Syria Anas Anbari, MD, PhD | Department of Ophthalmology, Mouassat University Hospital, Damascus University, Damascus, Syria
|
|
|
| Abstract | | We report the refractive correction of high astigmatism in one eye of a 23-year-old woman following deep anterior lamellar keratoplasty (DALK) using an Artisan iris-fixated, toric, phakic intraocular lens (IOL). One year after implantation, uncorrected and corrected distance visual acuities were both 20/25, refraction was −1.00 D cylinder, and the endothelial cell count was 1827 cells/mm2. Iris-fixated phakic IOLs are not recommended for every postkeratoplasty patient with high refractive error; however, this procedure can offer good outcomes in carefully selected cases of previous DALK. | | | Introduction | | Many patients experience high refractive error following keratoplasty. It can be corrected by spectacles, contact lenses, or corneal refractive surgery.(1) In some patients, however, these treatments are not appropriate; the presence of anisometropia can limit the use of spectacles, and contact lens intolerance may prevent their use. Excimer laser surgery offers less predictable results, may not fully correct the refractive error, and carries a relatively high rate of complications.(1) Cases that are not amenable to standard treatment modalities require an alternative method of refractive correction. We report our experience with a toric phakic intraocular lens (IOL) for the correction of high astigmatism in one eye of a single patient following deep anterior lamellar keratoplasty (DALK). | | | Case Report | A 23-year-old woman with keratoconus underwent big-bubble DALK in her left eye. Eighteen months after surgery, she presented with high astigmatism. On examination, uncorrected distance visual acuity in her left eye was 20/50; spectacle-corrected (+4.75 −5.00 × 60) distance visual acuity was 20/30. Keratometry readings were K1 = 41.50 × 60 and K2 = 46.50 × 150. Anterior chamber depth was 3.96 mm (measured from the epithelium to the crystalline lens). Mesopic pupil diameter was 4.1 mm (Sirius CSO; Costruzione Strumenti Oftalmici, Florence, Italy). Endothelial cell count was 2043 cells/mm2 (Topcon SP-2000P non-contact specular microscope, Topcon Corp, Tokyo, Japan).
She had undergone a penetrating keratoplasty (PKP) in her right eye 8 years previously, and her current refraction was −7.50 −3.50 × 35, and the endothelial cell count was 1249 cells/mm2. She was using soft contact lens to correct the right eye refractive error. She was intolerant to semirigid gas permeable contact lenses and intolerant to glasses due to the presence of anisometropia.
After discussing various options, including corneal refractive procedures, the patient opted for Artisan toric phakic IOL (Ophtec BV, Groningen, The Netherlands) implantation. A 5.0/8.5 mm, +6.00 −6.50 × 60 Artisan toric phakic IOL with the cylinder axis at 90° to the haptics was inserted uneventfully in the anterior chamber of her left eye through a biplanar, 5.2 mm, posterior corneal (limbal) incision on the flat corneal meridian. Care was taken to secure the lens accurately in the correct axis, and interrupted sutures were used to control postoperative astigmatism by selective postoperative limbal incision suture removal.
Uncorrected distance visual acuity in the left eye improved to 20/32 by 1 week after surgery and to 20/25 by 1 year, by which time best-corrected visual acuity was 20/25, with a refraction of −1.00 D cylinder × 30. Her keratometry readings were K1 = 41.75 × 60 and K2 = 46.50 × 150, and the endothelial cell count was 1827 cells/mm2. | | | Discussion | Artisan toric phakic IOLs have been used with good results for the treatment of refractive errors in otherwise healthy eyes,(2) with good rotational stability.(3) Artisan phakic IOLs have demonstrated safety in long-term follow-up studies.(4) Results vary with respect to endothelial cell loss with the Artisan phakic IOLs for the correction of ametropia after PKP.(5-6) In general, PKP patients show accelerated long-term endothelial cell loss compared to DALK patients, who have lower rates of long-term cell loss.(7)
Toric phakic IOL implantation was one of the options to manage this patient with high astigmatism, intolerance to both glasses and semirigid gas permeable contact lenses, and good visual potential, with best-corrected distance visual acuity of 20/30, which was an indication of a low irregular astigmatism in her case. The patient declined corneal refractive surgeries, knowing their limitations to fully correct her astigmatism and risk of complications.(1)
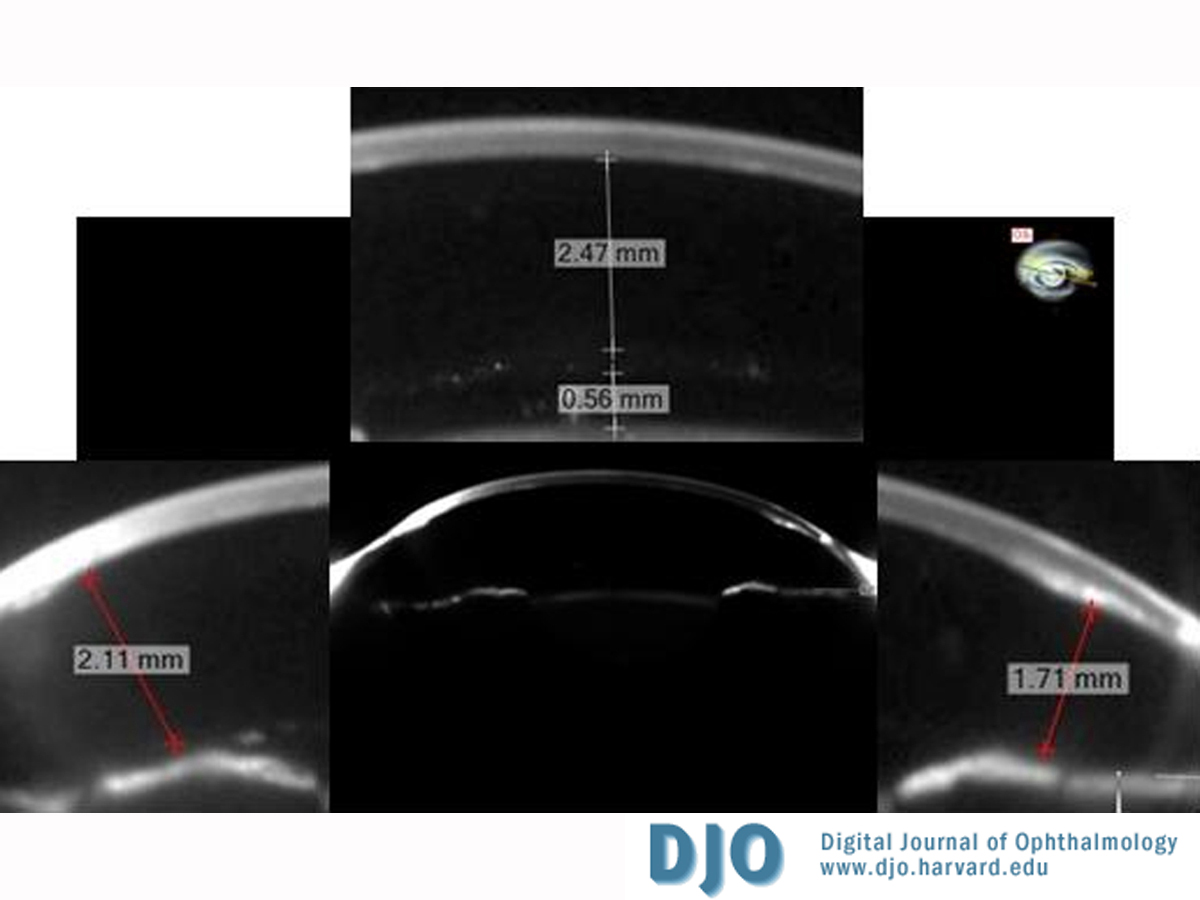
Artisan phakic IOLs have been demonstrated to be a safe option with respect to endothelial cell count, with a reported loss between 8.6% and 14.5% at 5 years.(8-10) In our case, the preoperative deep anterior chamber (3.96 mm) and the resultant postoperative critical distances (the distances between the optic edges of the phakic IOL and the corneal endothelium) of 1.71 mm and 2.11 mm (Figure 1) provided a safeguard against endothelial cell loss.(11) The preoperative and 1 year postoperative endothelial cell counts were 2043 cells/mm2 and 1827 cells/mm2, respectively (10.6% cell loss). The patient was very satisfied with the result.
To our knowledge, this is the first case report to describe the use of Artisan toric phakic IOL to correct high astigmatism after DALK. Tehrani and Dick have described the use of Artisan toric phakic IOLs for the correction of high astigmatism after penetrating keratoplasty.(12) Georgoudis and Tappin have reported the use of spherical Artisan phakic IOLs for the correction of ametropia after DALK.(13) Implantation of an Artisan toric phakic IOL can offer good visual outcomes in carefully selected cases of previous DALK with high astigmatism. The procedure is reversible, and in contrast to excimer laser corneal refractive surgery, there is no risk of postoperative haze and minor manipulation to the allograft, with no compromise to its structural integrity can be expected. Further long-term studies are needed to determine the rate of endothelial cell loss in these cases.
Literature Search
The authors conducted a MEDLINE search, without language restriction, using the PubMed database through February 2012. The following terms and combinations of terms were used: astigmatism AND deep anterior lamellar keratoplasty; deep anterior lamellar keratoplasty AND refractive errors; keratoplasty AND phakic intraocular lens OR toric phakic intraocular lens OR iris-fixated intraocular lens OR iris-claw intraocular lens OR iris-clip intraocular lens.
| |
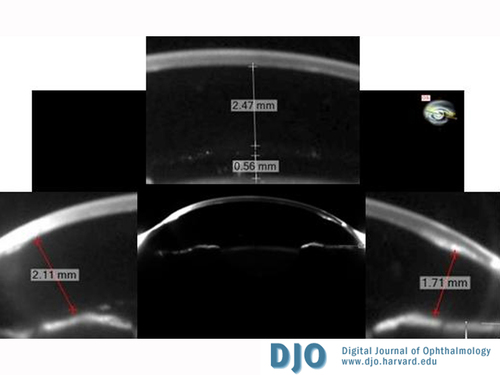
Figure 1
Toric phakic intraocular lens (IOL) distances from vital ocular structures (Sirius CSO; Costruzione Strumenti Oftalmici, Florence, Italy) showing the anterior segment of the patient’s eye and illustrating the measured distance between the anterior surface of the phakic IOL and corneal endothelium (2.47 mm), distance between the posterior surface of the phakic IOL and anterior surface of the crystalline lens (0.56 mm), and critical distances (1.71 mm and 2.11 mm).
|
|
| References | 1. Kollias AN, Schaumberger MM, Kreutzer TC, et al. Two-step LASIK after penetrating keratoplasty. Clin Ophthalmol 2009;3:581-6.
2. Güell JL, Vazquez M, Malecaze F, et al. Artisan toric phakic intraocular lens for the correction of high astigmatism. Am J Ophthalmol 2003;136:442-7.
3. Tehrani M, Dick HB, Schwenn O, et al. Postoperative astigmatism and rotational stability after Artisan toric phakic intraocular lens implantation. J Cataract Refract Surg 2003;29:1761-6.
4. Tahzib NG, Nuijts RM, Wu WY, Budo CJ. Long-term study of Artisan phakic intraocular lens implantation for the correction of moderate to high myopia: ten-year follow-up results. Ophthalmology 2007;114:1133-42.
5. Moshirfar M, Barsam CA, Parker JW. Implantation of an Artisan phakic intraocular lens for the correction of high myopia after penetrating keratoplasty. J Cataract Refract Surg 2004;30:1578-81.
6. Tahzib NG, Cheng YY, Nuijts RM. Three-year follow-up analysis of Artisan toric lens implantation for correction of postkeratoplasty ametropia in phakic and pseudophakic eyes. Ophthalmology 2006;113:976-84.
7. Borderie VM, Sandali O, Bullet J, et al. Long-term results of deep anterior lamellar versus penetrating keratoplasty. Ophthalmology 2012;119:249-55.
8. Saxena R, Boekhoorn SS, Mulder PG, et al. Long-term follow up of endothelial cell change after Artisan phakic intraocular lens implantation. Ophthalmology 2008;115:608-13.
9. Benedetti S, Casamenti V, Benedetti M. Long-term endothelial changes in phakic eyes after Artisan intraocular lens implantation to correct myopia: five-year study. J Cataract Refract Surg 2007;33:784-90.
10. Silva RA, Jain A, Manche EE. Prospective long-term evaluation of the efficacy, safety, and stability of the phakic intraocular lens for high myopia. Arch Ophthalmol 2008;126:775-81.
11. Doors M, Cals DW, Berendschot TT, et al. Influence of anterior chamber morphometrics on endothelial cell changes after phakic intraocular lens implantation. J Cataract Refract Surg 2008;34:2110-8.
12. Tehrani M, Dick HB. Implantation of an Artisan toric phakic intraocular lens to correct high astigmatism after penetrating keratoplasty. Klin Monatsbl Augenheilkd 2002;219:159-63.
13. Georgoudis P, Tappin MJ. Artisan phakic IOL for the correction of ametropia after deep anterior lamellar keratoplasty. J Refract Surg 2010;26:87. | |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in