|
|
 |
|
|
|
|
|
Orbit/Oculoplastics Quiz 6
|
Printer Friendly
|

 Carolyn Kloek, M.D. Carolyn Kloek, M.D. | Massachusetts Eye and Ear Infirmary | Massachusetts Eye and Ear Infirmary October 30, 2004
|
|
[Back to Questions] [Back to Orbit/Oculoplastics]
|
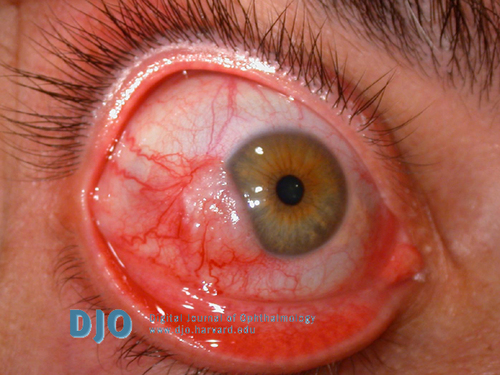
Figure 1
Clinical appearance at presentation
|
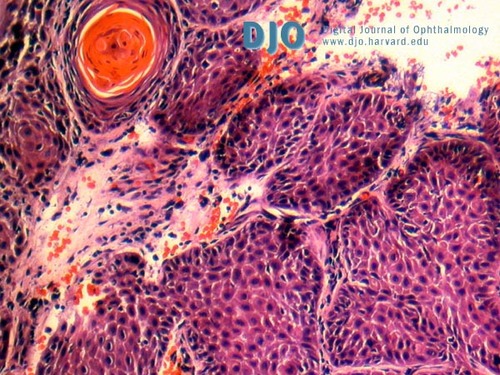
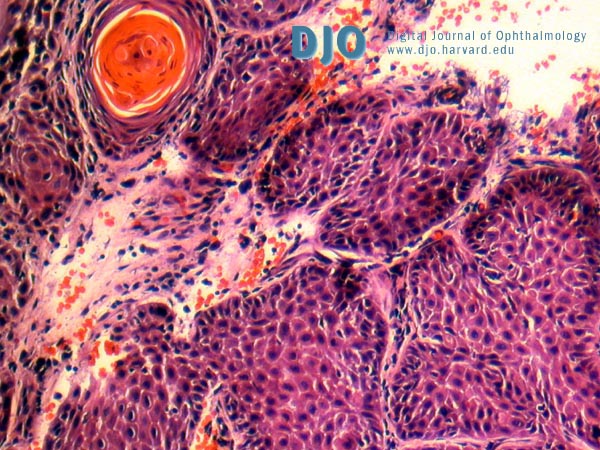
Figure 2
Pathology (hematoxylin and eosin stain) of biopsy of lesion shown in Figure 1.
|
| | Case History | | A 49-year-old male presents complaining of a slowly growing conjunctival lesion. | | | Questions and Answers | 1. What is the diagnosis?
Answer: Squamous cell carcinoma of the conjunctiva
2. What are the characteristic clinical and histologic features of this condition?
Answer: Squamous cell carcinoma of the conjunctiva presents as a fleshy, elevated lesion in the interpalpebral fissure abutting the limbus. Leukoplakia, a white plaque, may be present on the surface of the lesion. Large, dilated conjunctival vessels extending toward the tumor are often present.
Histopathologically, squamous cell carcinoma of the conjunctiva appears as neoplasia involving the full-thickness of the conjunctival epithelium, invading the basement membrane into the underlying stroma. Conjunctival intraepithelial neoplasia (CIN), a precursor to squamous cell carcinoma, is characterized by neoplasia involving only partial-thickness of the conjunctival epithelium and not invading the basement membrane. If untreated, CIN will often progress to invasive squamous cell carcinoma. Leukoplakia represents hyperkeratosis, dyskeratosis, and parakeratosis of the conjunctival epithelium.
Shields CL, Shields JA. Tumors of the conjunctiva and cornea.
Surv Ophthalmol. 2004 Jan-Feb;49(1):3-24. Review.
3. What is the etiology of this lesion?
Answer: The etiology of squamous cell carcinoma of the conjunctiva is likely multi-factorial. A correlation between incidence of squamous cell carcinoma of the conjunctiva and exposure to ultraviolet light has been noted. This link is supported by the fact that squamous cell carcinoma of the conjunctiva usually arises in the interpalpebral fissure, the portion of conjunctiva most frequently exposed to light.
Similar to squamous cell carcinoma of the cervix, human papilloma virus (strains 16 and 18) is thought to play a role in the development of squamous cell carcinoma of the conjunctiva in some individuals, particularly those affected by bilateral disease.
An increased frequency of squamous cell carcinoma of the conjunctiva has been observed in immunocompromised patients, particularly those with HIV. If a young individual presents with bilateral squamous cell carcinoma of the conjunctiva, an immunocompromised condition must be suspected.
Yoon YD, Grossniklaus H. Tumors of the cornea and conjunctiva. Curr Opin Ophthalmol. 1997 Aug;8(4):55-8. Review.
4. What is the clinical course of this condition?
Answer: Squamous cell carcinoma of the conjunctiva most commonly spreads superficially, extending into the conjunctival stroma and corneal epithelium. If untreated for an extensive period of time, the tumor can invade into the sclera, anterior chamber, and/or orbit. Metastases can occur, usually initially affecting regional lymph nodes followed by distant spread.
Tunc M, Char DH, Crawford B, Miller T. Intraepithelial and invasive squamous cell carcinoma of the conjunctiva: analysis of 60 cases. Br J Ophthalmol. 1999 Jan;83(1):98-103.
5. What are the treatment options?
Answer: Excisional biopsy is recommended for conjunctival lesions suspected of being squamous cell carcinoma. The conjunctival portion of the lesions should be excised with wide margins (at least 4mm) of normal conjunctiva, along with a thin lamella of underlying sclera. Cryotherapy can be applied at the edges of tumor resection in an attempt to destroy remaining tumor cells. If corneal involvement is suspected, alcohol epitheliectomy can be applied to denude the corneal epithelium to Bowman’s layer.
If the tumor is only partially excised or the tumor recurs after primary excision, adjunctive therapy with mitomycin-C or 5-fluoruracil can be used post-operatively to treat residual intraepithelial disease. Deeper residual or recurrent disease is best treated with further surgical resection.
If extensive intraocular or orbital involvement is present at the time of diagnosis, orbital exenteration is often recommended.
Peksayar G, Altan-Yaycioglu R, Onal S. Excision and cryosurgery in the treatment of conjunctival malignant epithelial tumours. Eye. 2003 Mar;17(2):228-32.
Shields CL, Naseripour M, Shields JA. Topical mitomycin C for extensive, recurrent conjunctival-corneal squamous cell carcinoma. Am J Ophthalmol. 2002 May;133(5):601-6.
Frucht-Pery J, Rozenman Y, Pe'er J. Topical mitomycin-C for partially excised conjunctival squamous cell carcinoma. Ophthalmology. 2002 Mar;109(3):548-52.
| | | [Back to Questions] |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in