|
|
 |
|
|
|
|
|
Glaucoma Quiz 7
|
Printer Friendly
|
|
|
|
[Back to Questions] [Back to Glaucoma]
|
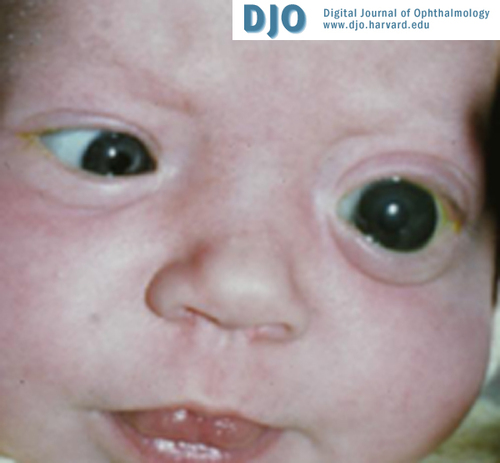
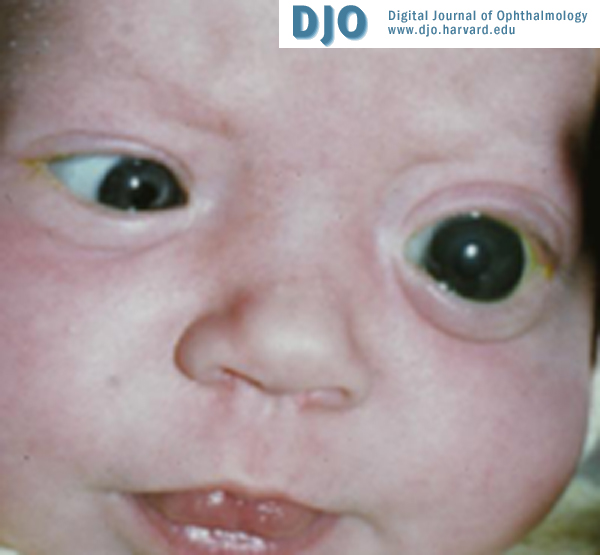
Figure 1
|
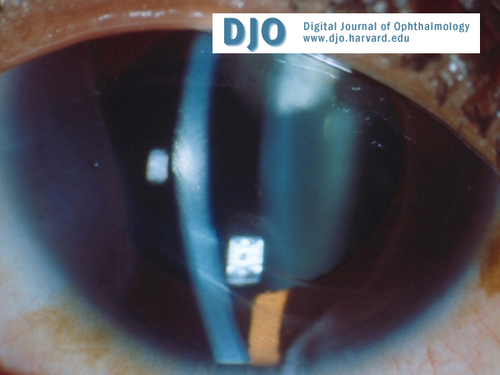
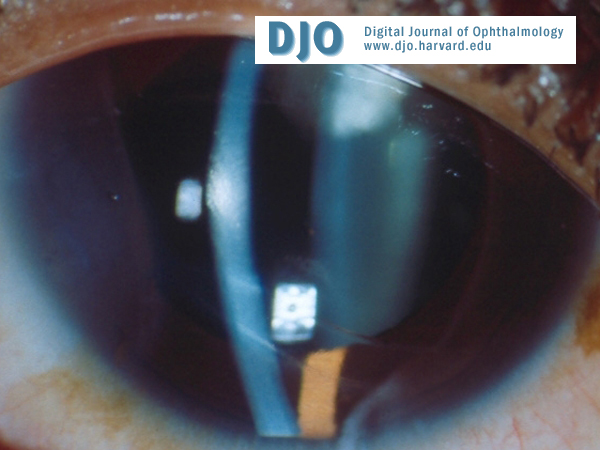
Figure 2
Haab's striae
|
| | Case History | A 3-month-old male infant was noted to have tearing from the left eye, which had a pressure of 48 mm Hg (Figure 1).
| | | Questions and Answers | 1. What type of glaucoma is this?
Answer: Primary congenital glaucoma, infantile glaucoma.
2. What is the pathophysiology?
Answer: Embryologically, there is an arrest in the migration and development of the neural crest cells that form the angle of the anterior chamber. This leads to angle malformation resulting in high intraocular pressure (IOP).
3. What are the breaks in Descemet’s called? How are they different from lines caused by birth trauma?
Answer: Haab’s striae. These are horizontal or concentric, single or multiple, parallel lines in the cornea caused by tears in Descemet’s membrane (Figure 2).
In contrast, birth trauma causes vertical or oblique tears in Descemet’s membrane.
4. What is the classic presentation?
Answer: The three classic symptoms are epiphora, photophobia, and blepharospasm. The signs and symptoms are mainly due to the high IOP. Patients may have buphthalmos, enlarged corneal diameters, corneal edema, Haab’s striae, and progressive myopia. Optic nerve cupping and angle abnormalities may be seen. The eye is susceptible to rupture on blunt trauma.
5. What is the inheritance pattern?
Answer: Many cases are sporadic. A polygenic inheritance pattern may be present. 10% - 40% are autosomal recessive.
6. What is the gonioscopic appearance?
Answer: In congenital glaucoma, there is classically anterior insertion of the iris, a stippled and irregular trabecular meshwork surface, and decreased transparency of tissues at the level of scleral spur and ciliary body band. The angle is usually open.
7. What is the differential diagnosis?
Answer: The differential diagnosis may include nasolacrimal duct obstruction, megalocornea, birth trauma, sclerocornea, congenital hereditary corneal dystrophy, keratitis, axial myopia, mucopolysaccharidosis, cystinosis, and tyrosinemia.
8. What is the work-up of these patients?
Answer: Work-up includes careful medical and ocular examination. Particular attention should be directed to corneal diameter measurements, cycloplegic refraction, and gonioscopy.
An examination under anesthesia may be needed.
9. What is the definitive treatment?
Answer: The treatment is usually surgical. The optic nerve cupping may be reversible in the early stages. Goniotomy, from an ab interno approach, is preferable in children with clear corneas. Trabeculotomy, or an ab externo approach, may be needed in children with hazy corneas. If these fail, filtration surgery, tube implant surgery, or cyclodestruction may be tried.
Medical treatment is usually a temporizing measure prior to surgical treatment.
| | | [Back to Questions] |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in