|
|
 |
|
|
|
|
|
Pathology Quiz 9: Lesion
|
Printer Friendly
|

Aaron Fay, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School Peter A.D. Rubin, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School March 8, 1999
|
|
[Back to Questions] [Back to Pathology]
|

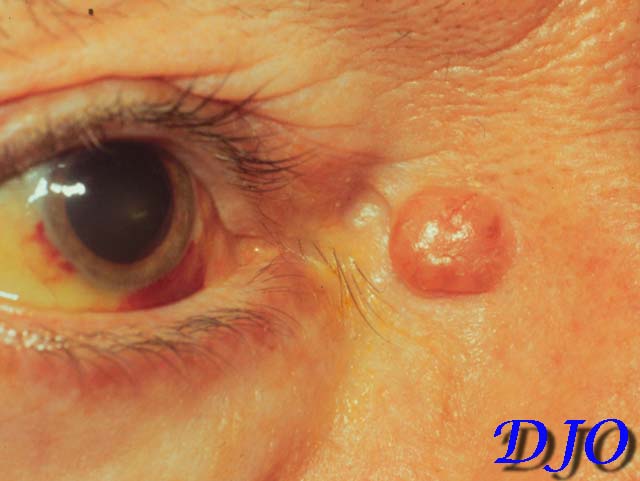
Figure 1
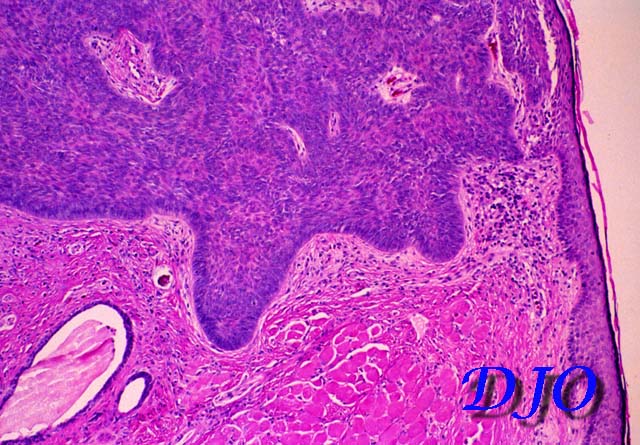
Figures 1-2. Clinical Photo and Histology.
|

Figure 2
|
| Questions and Answers | 1. Describe the clinical appearance of this lesion.
Answer: The clinical photograph demonstrates a well demarcated 8 mm, lightly pigmented, right medial canthal nodule. The nodule is pearly in texture and is centrally umbilicated with fine telangiectasias on the surface. There is no edema, erythema, ulceration, necrosis, hemorrhage or associated conjunctivitis.
2. Describe the histologic characteristics of this lesion.
Answer: The specimen consists of keratinizing squamous epithelium on the top with underlying dermis. Invading the stroma is a well-circumscribed collection of uniform, coherent, and deeply basophilic cells arising FROM the epithelium. The cells at the periphery of the lesion are aligned in picket fence formation, an arrangement known as ìperipheral palisading.î There is artifactual clefting between the tumor and surrounding tissues.
3. Name three entities in the differential diagnosis.
Answer: Answer:
- dermal nevus
- hemangioma
- epidermal inclusion cyst
- squamous cell carcinoma
- basal cell carcinoma.
4. What is the diagnosis?
Answer: basal cell carcinoma, nodular pattern.
5. What is the natural history of this lesion?
Answer: Basal cell carcinoma (BCC) is the most common skin cancer in human beings accounting for 90% of eyelid skin cancers. It is found in adults with increasing frequency with advancing age. Fair skinned individuals are at greatest risk and the disease is virtually unknown among heavily pigmented peoples. Actinic exposure confers an increased risk as does radiation exposure, xeroderma pigmentosum, and the nevoid basal cell carcinoma syndrome (autosomal dominant).
The most common periocular location is the lower eyelid, followed by medial canthus, upper eyelid, and lateral canthus. Most common is the nodular form of BCC; other clincal variants include cystic, necrotic, sclerosing, and pigmented forms. While metastasis is rare, local invasion (especially with recurrent lesions) can be aggressive and destructive. Medial canthal or lateral canthal lesions have a propensity for orbital invasion and may require radiographic imaging prior to excision.
6. What is the treatment of choice?
Answer: The treatment of choice is complete surgical resection. This may be accomplished with traditional excisional techniques in primary lesions. Frozen section control is not usually employed in nodular surface lesions because histologic margins correlate highly with the clinical LIMIT of the lesion. Mohs micrographic surgery may be the method of choice for poorly defined lesions (i.e. sclerosing variant) or for recurrent lesions in which the anatomic planes have been disrupted, especially medial/lateral canthal lesions where the potential for orbital invasion is greatest.
| | | [Back to Questions] |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in