|
|
 |
|
|
|
|
|
Orbit/Oculoplastic Quiz 4
|
Printer Friendly
|

Ramin Tayani, M.D., M.P.H. | Massachusetts Eye and Ear Infirmary, Harvard Medical School Aaron Fay, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School Peter A.D. Rubin, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School November 7, 1998
|
|
[Back to Questions] [Back to Orbit/Oculoplastics]
|
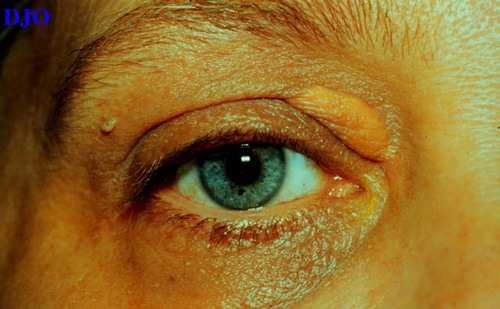
Figure 1
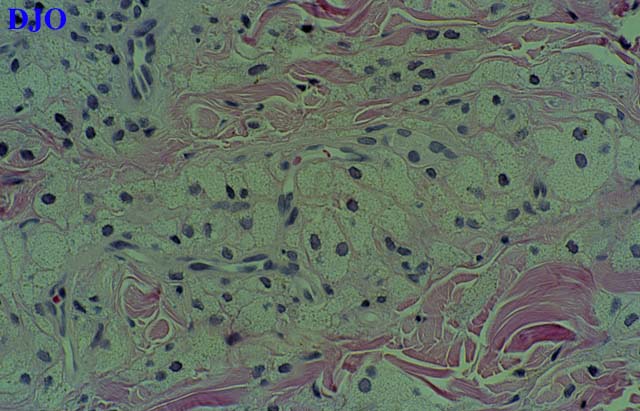
Figures 1-2. Clinical Photo and Histology.
|

Figure 2
|
| Questions and Answers | 1. What is the diagnosis?
Answer: Xanthelasma.
2. What is the most common systemic abnormality of this disease?
Answer: No disease! Two thirds of patients with xanthelasma are normolipemic. But it can occur in all five of the subtypes of essential hyperlipidemia (especially types II and III). Also, can be seen in diseases associated with secondary hyperlipidemia (e.g. diabetes mellitus, primary biliary cirrhosis).
3. What are the clinical and histologic manifestations?
Answer: Most commonly, in middle-aged or elderly individuals. It appears as multiple, soft, yellowish plaques most commonly at the inner aspects of the upper and lower lids. It is a form of xanthoma i.e. a tumor containing fat mainly within cells (intracellular), whereas a lipogranuloma, e.g. a chalazion, is a tumor containing fat mainly outside of cells (extracellular). Histologically, lipid containing foam cells (lipid-laden histiocytes) are found in the superficial dermis. The cells cluster around blood vessels and may even involve their walls.
4. What other disease has similar lesions?
Answer: Erdheim-Chester disease, which is an idiopathic, widespread, multifocal, granulomatous disorder characterized by cholesterol-containing foam cells infiltrating viscera and bones, including the orbit, and sometimes bilateral xanthelasmas.
5. How are these lesions treated?
Answer: Observation, surgical excision, ablation: carbon dioxide laser or topically with 100% trichloroactic acid. Care should be taken with surgical excision since these lesions may recur, and with recurrent lesions and excisions one may get a cicatritial ectropion involving the anterior lamella.
| | | [Back to Questions] |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in