Figure 1
This is a patient who complained of blurry vision in his right eye over one week associated with pain with eye movements and a central scotoma. He had a right afferent pupillary defect and dyschromatopsia OD.
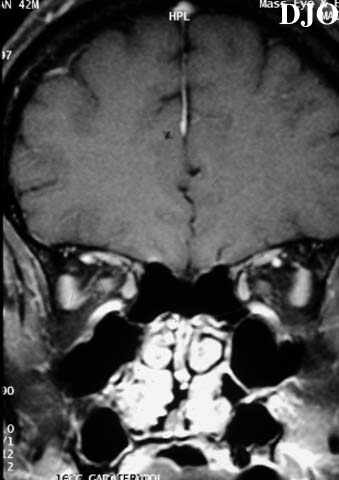
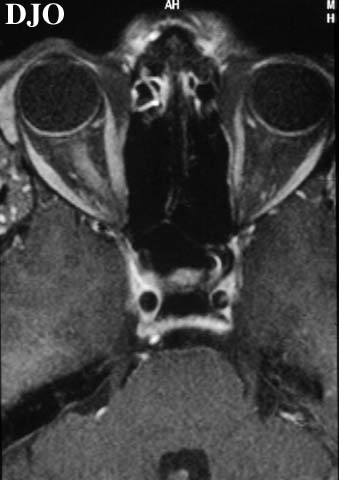
Figure 2
Figures 2-3. This patient's axial and coronal MRI scans showed increased signal in the right optic nerve on T1 weighted imaging
Figure 3
Questions and Answers
1. What is the most likely diagnosis? Answer: Retrobulbar optic neuritis is the most likely diagnosis given the overall clinical presentation. The MRI scans showing increased signal intensity on T1 weighted images of the right optic nerve is also consistent with optic neuritis. Notably, no mass is seen compressing the optic nerve.
2. What is the natural history of this condition? Answer: Patient's usually have worsening of vision for up to 14 days. Typically, thereafter the visual acuity improves over several weeks. Approximately 85% of all patients with their first attack of optic neuritis will have recovery to 20/40 or better vision. However, when the presenting visual acuity is worse than 20/200 the chance of recovery to better than 20/40 falls to only 1/3 of patients.
3. With what systemic disease is the above condition most closely associated? How strong is this association? Answer: Multiple sclerosis. Several studies have confirmed a strong association between optic neuritis and multiple sclerosis. This risk is approximately 75% in women after 15 years and 40% in men after 15 years.
4. What is the value of MRI in the evaluation of this condition? Answer: MRI is useful to exclude compressive causes of optic neuropathy and to confirm the presence of an optic neuritis. MRI is also very helpful to look for multiple periventricular white matter lesions which are characteristic of multiple sclerosis.
5. What route and dosage of steroids may be beneficial in this condition? Answer: The Optic Neuritis Treatment Trial showed that I.V. steroids have a role in patients with MRI scans that are compatible with multiple sclerosis. In these patients I.V. methlyprednisolone (250 mg TID for 3 days) decreased the risk of developing multiple sclerosis for the first 2 years following the initial attack of optic neuritis. I.V. steroids have also been shown to slightly speed recovery of vision in optic neuritis, but the final visual acuity is the same with or without I.V. steroids. An important point is that oral steroids are contraindicated since they were found to increase the chance of repeat attacks of optic neuritis.
 Welcome, please sign in
Welcome, please sign in