|
|
 |
|
|
|
|
|
Cornea/Refractive Surgery Quiz 24
|
Printer Friendly
|

Yichieh Shiuey, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School December 14, 1998
|
|
[Back to Questions] [Back to Cornea/Refractive Surgery]
|
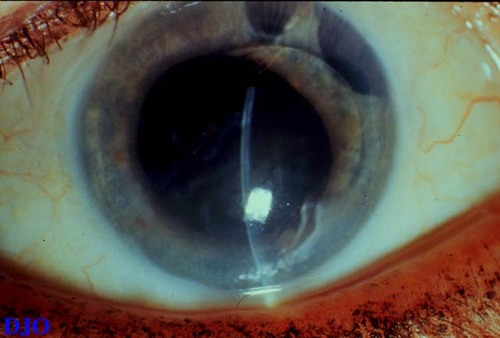
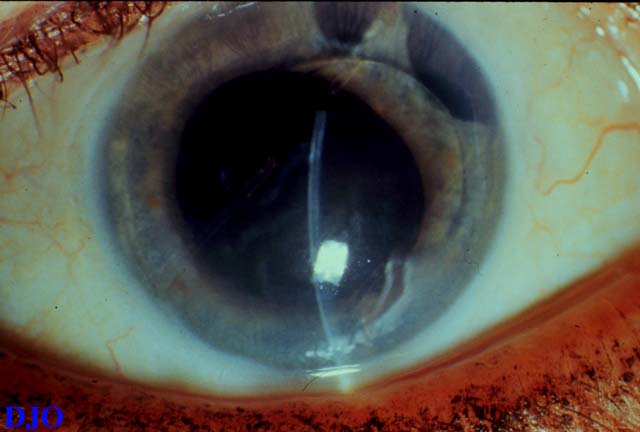
Figure 1
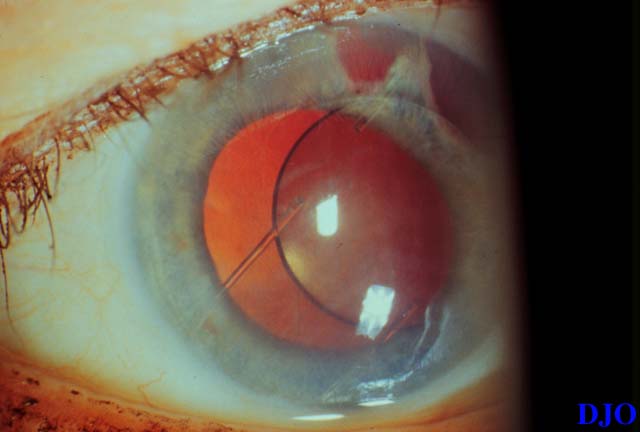
Figures 1-2. This patient had an intracapsular cataract extraction and placement of an anterior chamber intraocular lens in 1980. She complains of progressively worsening vision in the right eye. The photograph on the right shows a slit beam through the cornea which demonstrates corneal edema and Descemet's folds. The photograph on the right shows a view of the right eye in retroillumination.
|
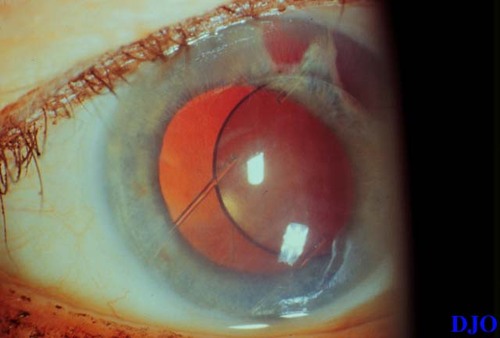
Figure 2
|
| Questions and Answers | 1. What is the diagnosis?
Answer: Pseudophakic bullous keratopathy (PBK).
2. What type of anterior chamber lens is present?
Answer: The patient has a Leiske closed-loop rigid anterior chamber lens.
3. Does the type of anterior chamber lens affect the likelihood of developing this condition?
Answer: Yes, the type of anterior chamber lens will affect the likelihood of developing PBK. Rigid closed loop lenses, such as those of the Leiske style, have a very high incidence of corneal decompensation. In contrast, modern flexible open loop anterior chamber lenses have a very low rate of corneal decompensation and PBK.
4. What is the pathophysiology of this conditon?
Answer: Rigid closed-loop anterior chamber lenses tend to move within the angle. The rigid closed loops are capable of rubbing against the peripheral endothelium, which causes the death of these peripheral endothelial cells. The response of the cornea to this injury is to enlarge the central corneal endothelial cells to cover the area of denuded peripheral endothelium. (Corneal endothelial cells cannot proliferate in adulthood.) Eventually, there are insufficient numbers of central endothelial cells to preserve the compactness and clarity of the cornea and PBK ensues.
5. What types of treatment may be indicated for this condition?
Answer: If the PBK is mild e.g. not yet affecting vision, the rigid closed loop anterior chamber lens should be removed to prevent progression of the PBK. A modern flexible anterior chamber lens or a scleral sutured posterior chamber intraocular lens may be placed at the time of surgery. An aphakic contact lens is another option. If the PBK is producing corneal edema with associated decreased vision or pain, penetrating keratoplasty with lens exchange is indicated.
| | | [Back to Questions] |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in