|
|
 |
|
|
|
|
|
Cornea/Refractive Surgery Quiz 17
|
Printer Friendly
|

Yichieh Shiuey, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School Kathy Colby, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School Claes Dohlman, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School February 26, 1997
|
|
[Back to Questions] [Back to Cornea/Refractive Surgery]
|

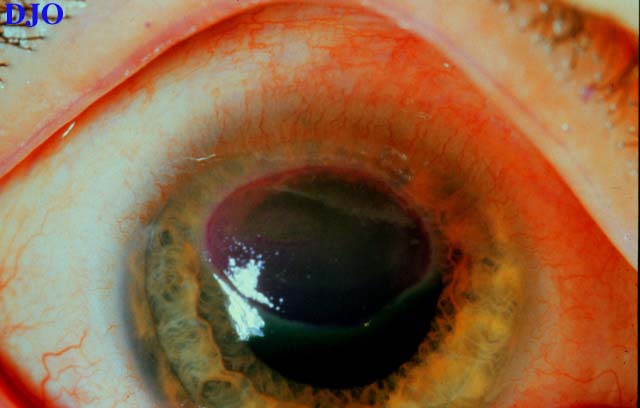
Figure 1
Figures 1-2. This is the right eye of a 19 year old man with history of severe itching OU and photophobia. He has no history of contact lens use.
|
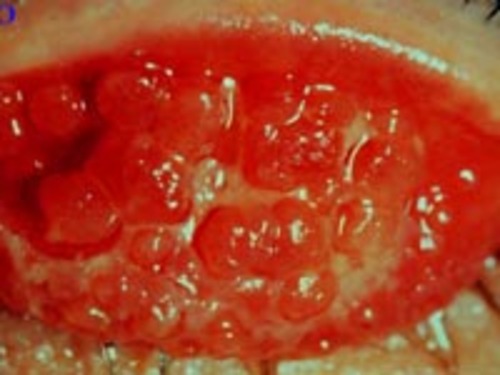
Figure 2
|
| Questions and Answers | 1. What is your diagnosis?
Answer: Vernal keratoconjunctivitis. (VKC) The large cobblestone papillae on the upper lid and the presence of a sterile shield ulcer in a teenage male is essentially pathognomonic of this diagnosis
2. What is the epidemiology of this condition?
Answer: VKC occurs more often in warm climates. There is a male predominance with a male to female ratio of at least 2:1. Onset of the condition is frequently at puberty with remission occuring often by the late teens.
3. What systemic conditions are associated with this diagnosis?
Answer: It is often associated with a history of atopic disease such as asthma, allergic rhinitis, and eczema.
4. What is the pathophysiology of this condition?
Answer: VKC is an allergic disease where mast cells and eosinophils are believed to play critical roles.
5. What pathologic finding is highly characteristic of this condition?
Answer: The presence of 2 or more eosinophils per high power field in a biopsy of conjunctiva is essentially pathognomonic of VKC.
6. How would you manage this condition?
Answer: The first step in treating VKC, as well as all other allergic conditions of the eye, is to identify the allergen. Once the allergen is identified, the patient can then learn to eliminate or avoid the antigen. The aid of an allergist may be very helpful in this regard. Topical therapy may include brief courses of steroids (up to several weeks) to quiet the disease, followed by rapid tapering. Mast cell stabilizers e.g. cromolyn and lodoxamide should be started while the patient is receiving steroids for acute flares since these agents require time for their clinical effects to occur. Once the acute situation is controlled some patients are able to be successfully treated with mast cell stabilizers alone. Other drugs that are being tried include cyclosporine and levocabastine. As was noted above, VKC often spontaneously remits after the late teens.
| | | [Back to Questions] |
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in