Lucas Maischner | Kings College Hospital Kashif Qureshi | St George's Hospital Fiona Robinson | Kings College Hospital Scott Robiee | St George's Hospital Shahram Kashani | Kings College Hospital Neelanjana Dutt | Kings College Hospital
Radiographic Studies
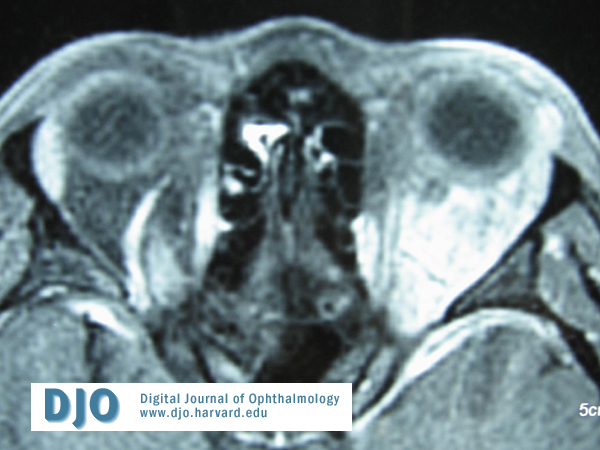
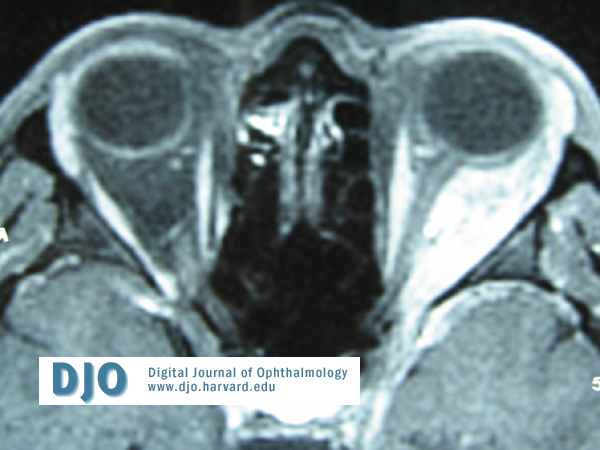
Magnetic Resonance Imaging demonstrated an abnormal ill defined mass filling the left retro orbital space. The abnormal mass extends from the globe to the orbital apex involving some extraocular muscles in particular the lateral rectus.
The abnormal mass appears to extend into the sclera and perhaps through the orbital apex where there may be increased enhancement around the para cavernous area and the anterior temporal lobe on the left .
The optic nerve was surrounded with this abnormal mass but had retained its CSF sheath. There was no paranasal sinus involvement and the right orbit was normal (figure 4 and 5) .
Pathology
Blood tests :
Full Blood Count plus differential , Urea and electrolytes and Autoantibodies were all normal. Anti Neutrophil Cytoplasmic Antibody (ANCA) was positive.
Orthoptic assessment :
The Humphrey threshold 30-2 visual fields were normal .
Hess chart demonstrated hypotropia of the left eye with limitation of upgaze as found on ocular motility (figure 3). The binocular single visual field was present only in the lower part of the visual field.
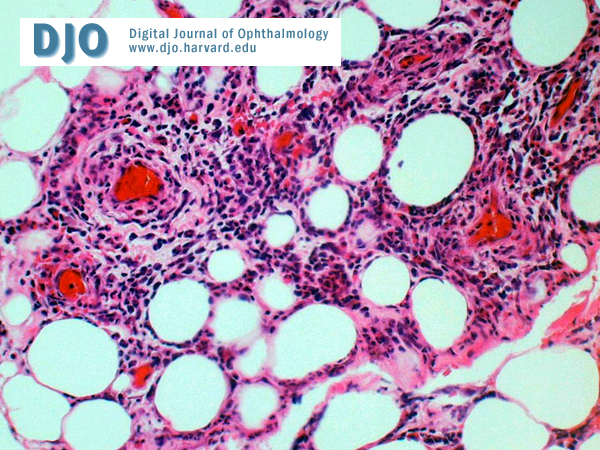
Histopathology :
Biopsy of the orbital lesion revealed several foci of perivascular inflammation .
The inflammatory cells appear to spill over into the adjacent fat lobules.
There was neutrophilic transmigration through the vessel walls. The closest differential on morphology is that of a panniculitic type of a T cell lymphoma which was ruled out .
The histological features were compatible with a diagnosis of Wegener’s Granulomatosis (figure 6) .
 Welcome, please sign in
Welcome, please sign in