|
|
A 5 year old girl who failed her school vision screening
Digital Journal of Ophthalmology 2004
Volume 10, Number 5
February 19, 2004
|
Printer Friendly
|
|
|
|
|
|
|
| Examination |
Her visual acuity was Count Fingers OD and 20/30 OS. There was no afferent pupillary defect. Her cycloplegic refraction was -1.50 +2.50 x 095 in the left eye, but no measurable retinoscopic light reflex could be appreciated in the right eye. She suppressed the right eye by Worth four-dot testing, but the eyes were orthotropic. The intraocular pressure was within normal limits.
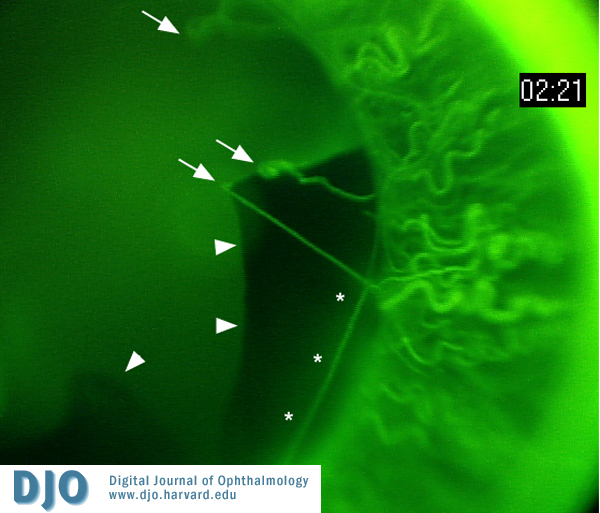
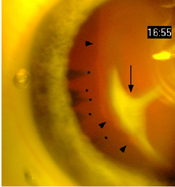
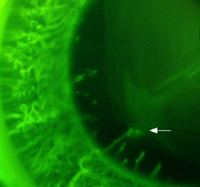
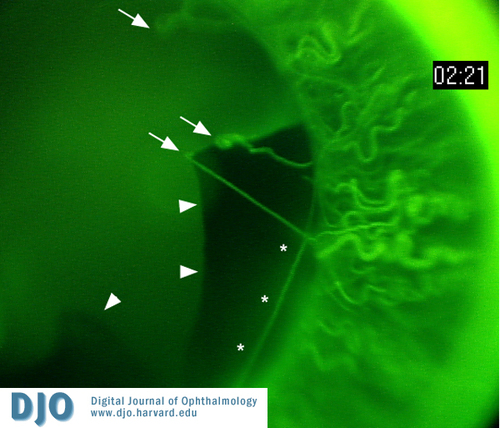
The slit lamp exam was remarkable for several distinctive findings in each eye. The right eye had a crescent-shaped, equatorial, fibrovascular plaque on the anterior lens capsule with a finger extending to the center of the optical axis of the capsule, causing distortion and capsular striae. There was central dragging of the ciliary processes and medial subluxation of the lens (Figure 1). Numerous remnants of the tunica vasculosa lentis (TVL) were present, and an anterior TVL vessel extended from the iris to the anterior surface of the plaque. The iris vasculature appeared engorged and contained many radial corkscrew vessels (Figure 2). There were vessels in the angle and also areas of angle closure. The left eye showed a broad area of iris pigment epithelial adhesion to the anterior lens capsule with persistent pupillary hairpin vessels present temporally (Figure 3). An elongated hairpin annular iris vessel was also seen extending across the superior pupil. Similar engorged corkscrew iris vessels were present. Perfused remnants of the posterior vasa hyaloidea propria and posterior TVL vasculature were seen in both eyes.
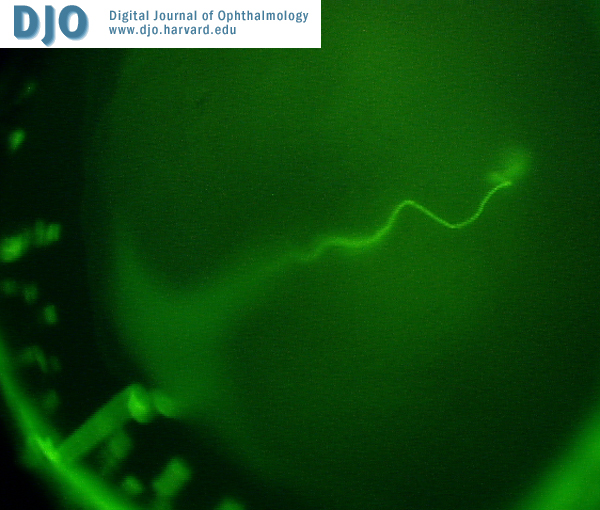
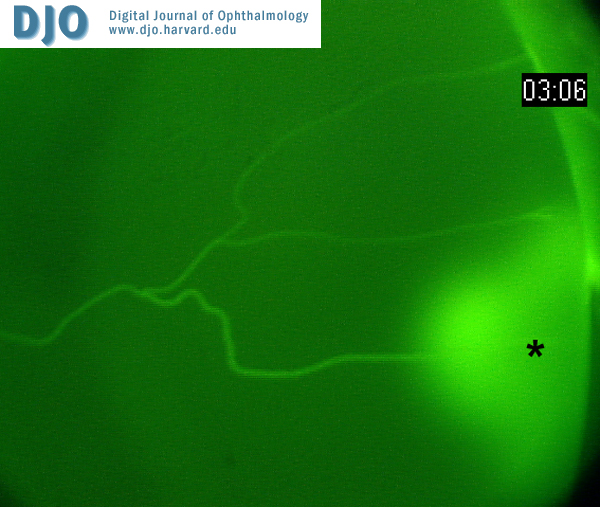
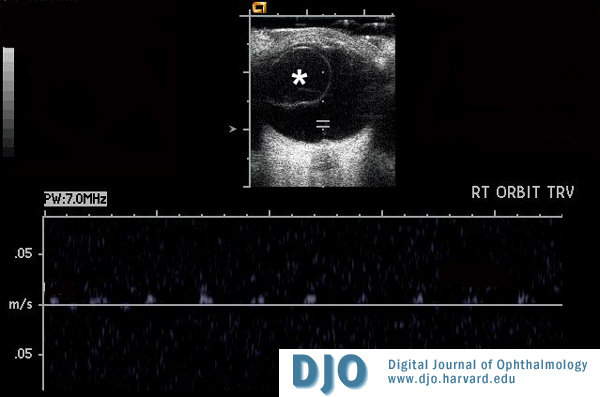
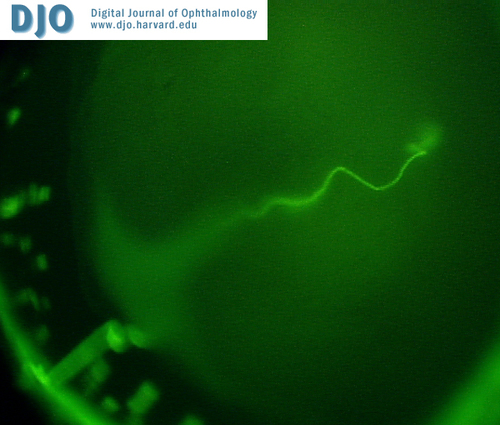
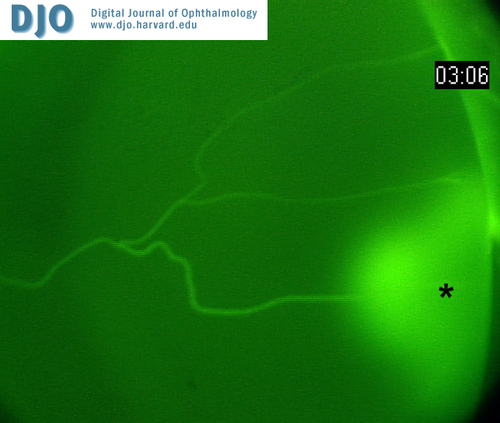
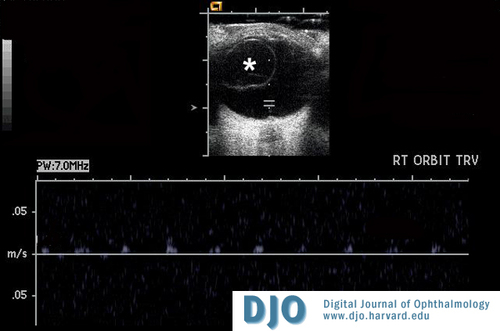
The posterior segment was evaluated by indirect ophthalmoscopy with fundus photography and fluorescein angiography using the RetCam (Massie Labs, Pleasanton, CA). The posterior segment findings were similar in both eyes. The maculas and peripheral retinas were normal in appearance, with well-developed foveas. There was a perfused hyaloid artery originating at the optic nerve head, which coursed anteriorly to the retrolental space. Fluorescein angiography demonstrated slow but complete perfusion of both hyaloid arterial trees (Figure 4). The hyaloid vessel then ramified into temporal coursing vasa hyaloidea vessels (1 in the right eye, 3 in the left eye), which anastomosed with the iris vasculature as described above. There was significant fluorescein leakage at the site of the anastomoses between these vessels in the left eye (Figure 4B). Anterograde flow was seen throughout the systems in both eyes except for an anastomosis in the left eye that showed retrograde perfusion from the iris back to a branch of the posterior tunica vasculosa lentis. Individual red blood cells could be seen flowing through the vessels of the posterior TVL on the angiogram study, consistent with a low-flow arterial system. Doppler ultrasound identified the hyaloid artery and measured the flow velocity within the artery in the mid-vitreous at 0.01-0.02 M/sec (Figure 5).
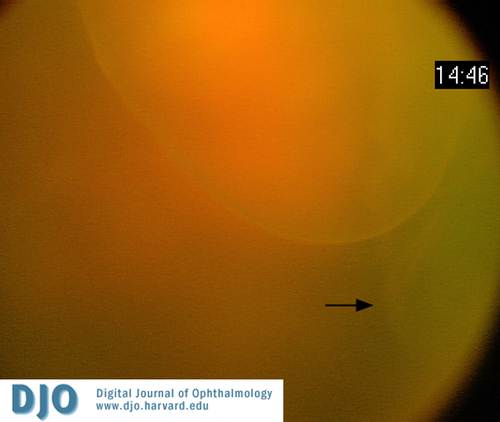
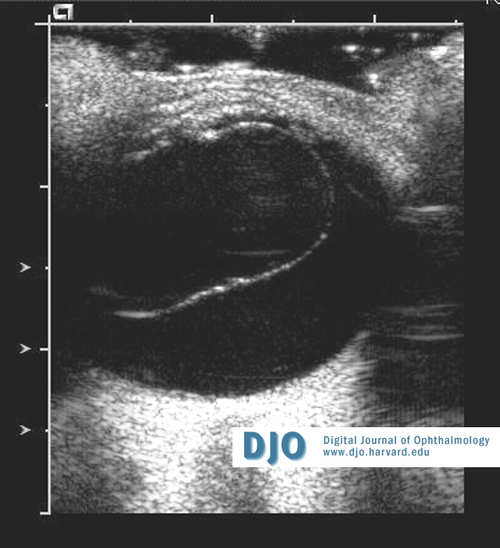
The vitreous was markedly abnormal in both eyes. In the right eye, the vitreous cavity appeared to be "optically empty" in the nasal hemisphere. There was an oval cystic structure in the vitreous cavity that was adherent to the hyaloid artery in the mid-vitreous (Figure 6). The cyst appeared to be anchored at the vitreous base temporally and was 1.0 x 1.6 cm in size by ultrasound (Figure 7). The left vitreous cavity also appeared to be "optically empty". Several translucent cystic masses were seen in the temporal periphery in the region of the vitreous base. One appeared to be a small oval mass of formed vitreous. Ultrasound studies showed these masses to be oval or spherical cysts within the vitreous cavity, each of which appeared to be anchored at the level of the vitreous base (Figure 8A). A hemispheric cyst fixed to the region of the vitreous base was also seen (Figure 8B). T2-weighted MRI images detected the large cyst in the left eye (Figure 9).
|
|
|
Figure 1
Figure 1. Plaque on the anterior lens capsule in the right eye (arrow). Medial subluxation of the lens and an irregular shape to the margin to the capsule are evident (arrowheads). Medial dragging of the ciliary body processes is also seen (asterisks).
 |
|
|
Figure 2
Iris vessels and vessels of the tunica vasculosa lentis (TVL) in the right eye. Several small remnants of the TVL are seen along the papillary margin. A single larger vessel anastomoses with vessels of the posterior TVL and vasa hyaloidea propria (arrow). Large radial corkscrew vessels are seen throughout the iris.
 |
|
|
Figure 3
Iris vessels and vessels of the tunica vasculosa lentis (TVL) in the left eye. A broad area of iris pigment epithelial adhesion to the anterior lens capsule is present (arrowheads). Elongated TVL vessels are dragged medially (arrows) and an annular iris vessel is also seen medial to the pupillary margin (asterisks). Large radial corkscrew vessels are seen throughout the iris.
 |
|
|
Figure 4a
Fluorescein angiogram of the right hyaloid arterial tree.
 |
|
|
Figure 4b
Fluorescein angiogram of the left hyaloid arterial tree. Dye leakage is seen at the inferior-most anastomosis of the posterior TVL (asterisk).
 |
|
|
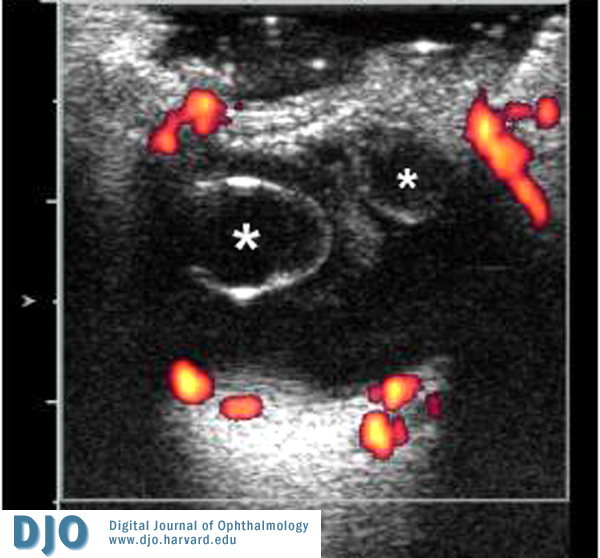
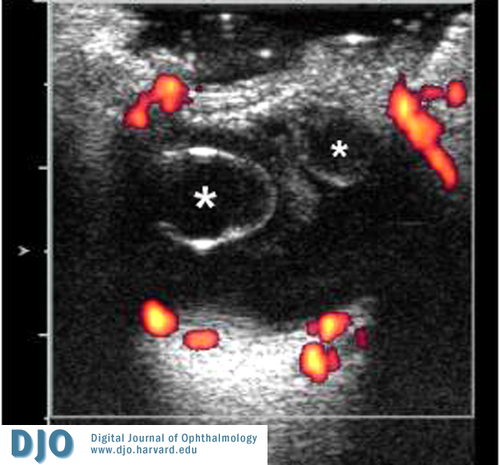
Figure 5
Dynamic ultrasound of the right eye. A large vitreous cyst is present in transverse section (asterisk). Flow analysis of the hyaloid artery in the posterior vitrous cavity demonstrates pulsatile arterial flow at 0.01-0.02 M/sec.
 |
|
|
Figure 6
RetCam image of the large vitreous cyst in the right eye. A smaller cyst appears to be present adjacent to it (arrow).
 |
|
|
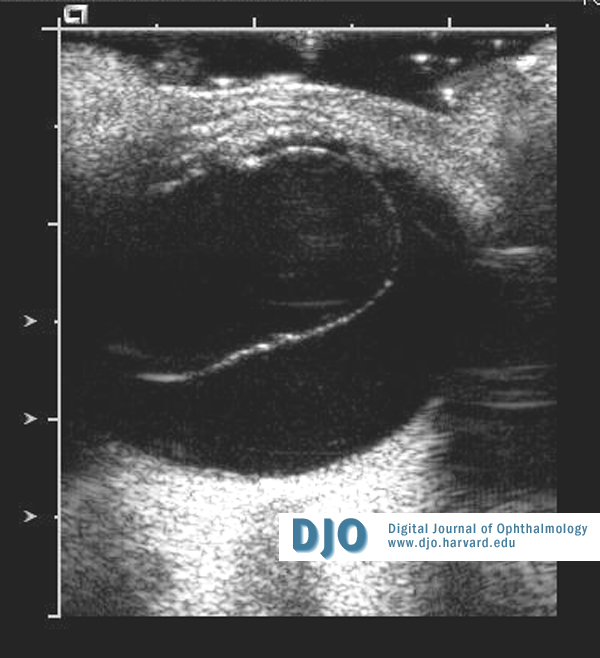
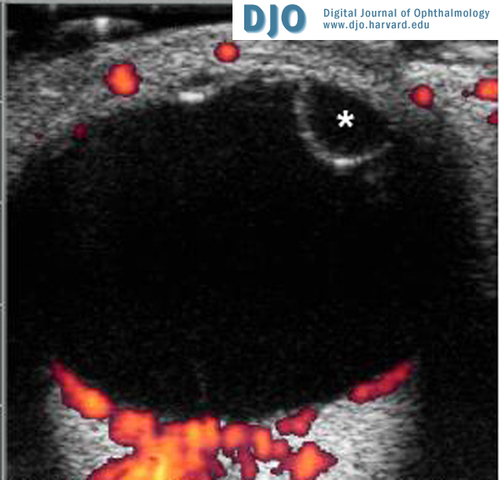
Figure 7
Ultrasound image of the right eye showing a large vitreous cyst in sagital section.
 |
|
|
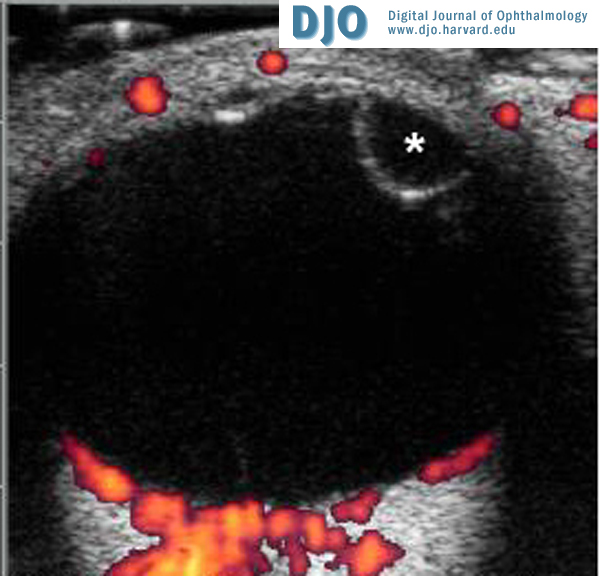
Figure 8a
Ultrasound studies showing multiple, small vitreous cysts in transverse section.
 |
|
|
Figure 8b
Ultrasound studiy showing hemispheric cyst at the vitreos base in the left eye.
 |
|
|
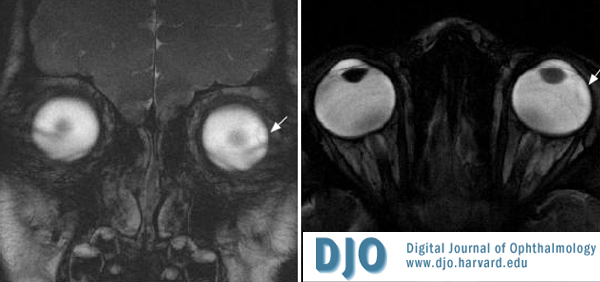
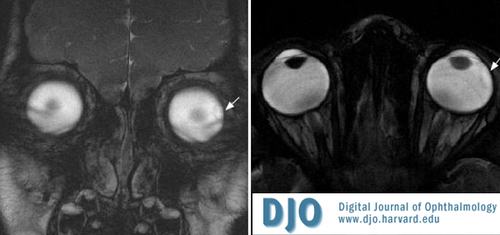
Figure 9
T2-weighted MRI images showing the large vitreous cyst in the left eye (arrows).
 |
|
 Welcome, please sign in
Welcome, please sign in