|
|
 |
|
|
|
|
|
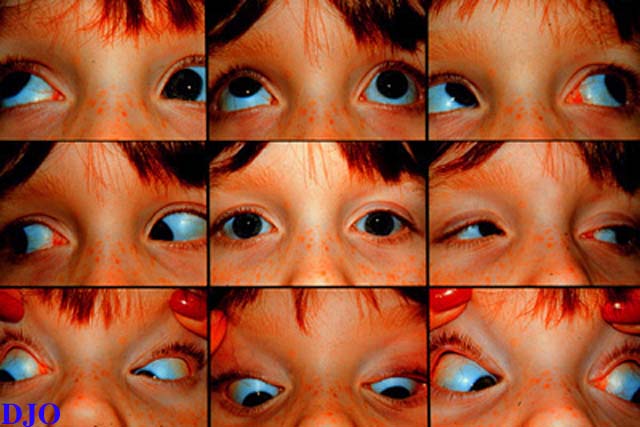
7 year old girl with a left face turn and binocular diplopia
Digital Journal of Ophthalmology 1997
Volume 3, Number 13
February 18, 1997
|
Printer Friendly
|
|
|

Mitchell S. Fineman, M.D. | Wills Eye Hospital, Philadelphia, PA Joseph Calhoun, M.D. | Wills Eye Hospital, Philadelphia, PA
|
|
|
| Differential Diagnosis | - Inferior oblique palsy: Characterized by negative forced duction test. The hypotropia would increase on ipsilateral head tilt.
- Blowout fracture: Secondary to tissue entrapment or scarring. Restriction to elevation in abduction and adduction is equal or greater in the field of action of the superior rectus. Forced duction positive.
- Superior oblique overaction:. Forced duction with free passive elevation, "A" pattern exotropia, and inferior oblique function is normal by duction.
- Congenital fibrosis syndrome: Bilateral, congenital, multiple EOM involvement including elevation deficiency, limitation of abduction and adduction and ptosis.
- Monocular elevation defect (double elevator palsy): Unilateral, congenital, elevation deficiency equal in abduction and adduction.
- Adherence syndrome: Follows surgery on the inferior oblique muscle. Restriction to elevation is greatest in lateral gaze.
Forced duction testing of the right eye revealed restriction to elevation in adduction. The left eye was normal. Therefore, the diagnosis of Brown's syndrome OD was confirmed. Treatment consisted of a right superior oblique tendon expansion with 6.0 mm silicone #40 retinal device. There were no surgical complications.
The postoperative course was complicated by diplopia in primary position. Motility revealed 16 PD right hypertropia in primary position and 20 PD right hypertropia in downgaze. A 4 PD right hypotropia was present in upgaze. The diplopia in primary gaze was successfully treated with a 13 prism diopter prism BD OD divided equally. Visual acuity was 20/25 OD and 20/20 OS.
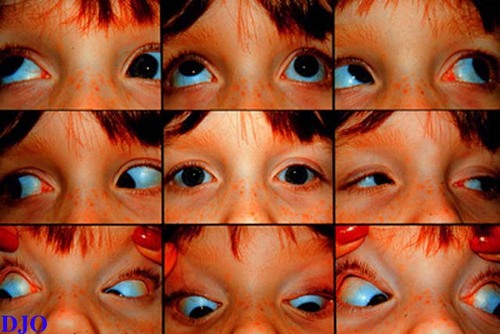
Ten months postoperatively, the patient presented to the Wills Eye Hospital Emergency Department after she noted the acute onset of binocular diplopia while wearing the corrective lenses . She denied a recent history of trauma or upper respiratory infection. There was no pain or tenderness. Examination of the extraocular motility is presented in Figure 2.
A right face turn of 10 degrees was also noted. Forced duction testing of the left eye revealed restriction of elevation in adduction. The diagnosis of a noninflammatory, atraumatic acquired left Brown's syndrome was made.
Medical evaluation including a complete physical examination, CBC, RF, and ANA was normal. A CT scan was performed. | |
|
Figure 2
Extraocular motility demonstrated by the diagnostic positions of gaze. Notable is the lack of elevation of the left eye when adducted.
 |
|
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in