|
|
 |
|
|
|
|
|
A 5-day-old-newborn with a large right upper eyelid coloboma
Digital Journal of Ophthalmology 2017
Volume 23, Number 3
September 28, 2017
DOI: 10.5693/djo.03.2017.08.001
|
Printer Friendly
Download PDF |
|
|

Dalia V. Zhang, BS | Cleveland Clinic Cole Eye Institute, Cleveland, Ohio Rao V. Chundury, MD, MBA | Glick Eye Institute, Indiana University, Indianapolis, Ohio Alexander D. Blandford, MD | Cleveland Clinic Cole Eye Institute, Cleveland, Ohio Julian D. Perry, MD | Cleveland Clinic Cole Eye Institute, Cleveland, Ohio
|
|
|
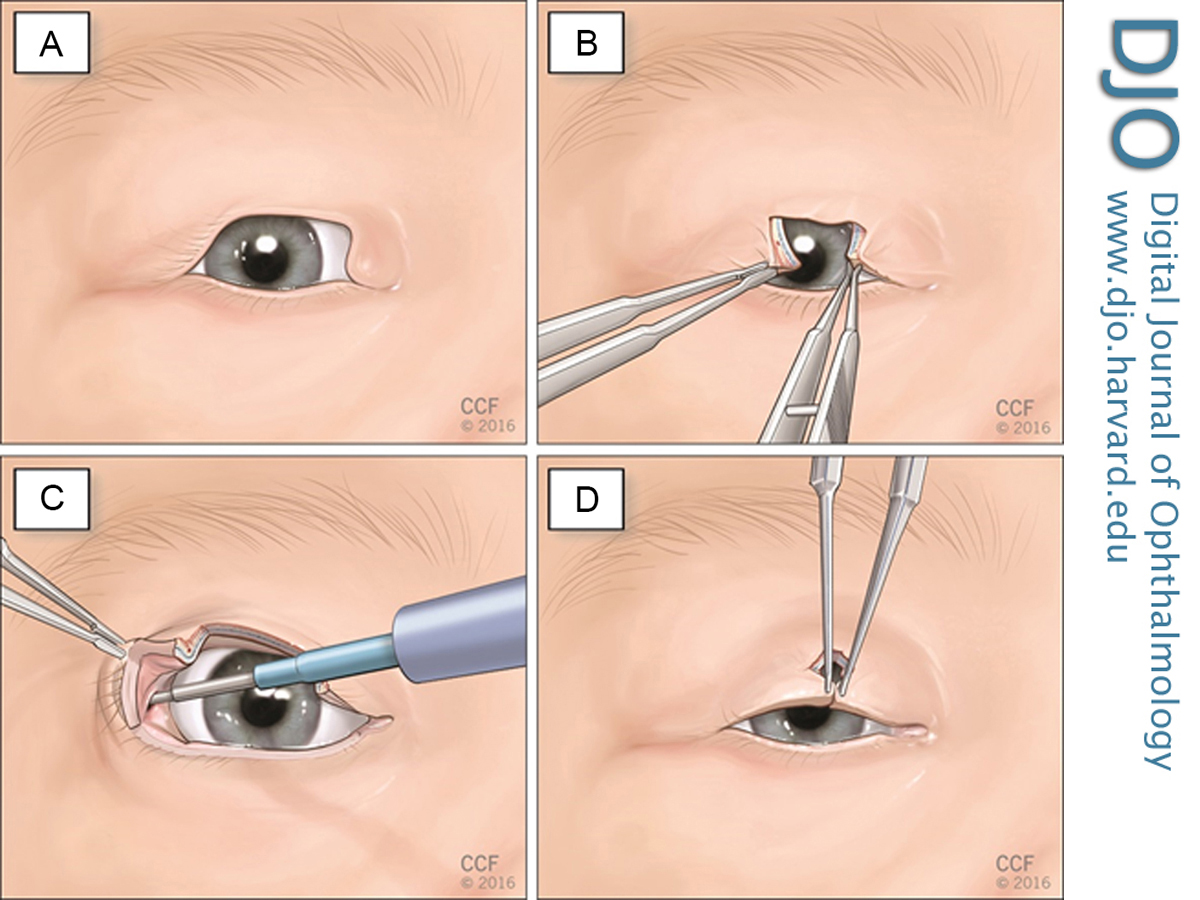
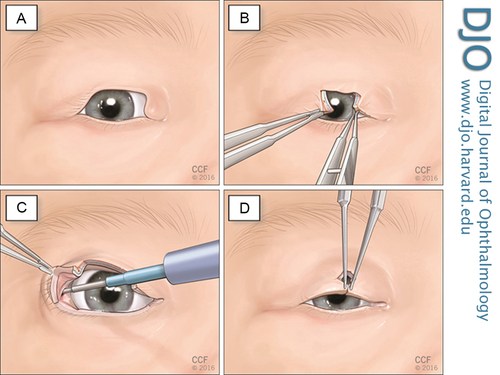
| Treatment | Under general endotracheal anesthesia, local anesthetic solution was injected into the lateral canthus and tissue surrounding the eyelid coloboma. This consisted of 1 ml of lidocaine 1% with 1:100,000 dilution of epinephrine and sodium bicarbonate 8.4% in a 1:10 ratio with 50 units per 10 ml of hyaluronidase. The coloboma borders were then squared, and direct approximation of the edges was attempted; however, correction via this method caused significant tension, resulting in ptosis. The internal cantholysis technique was then used to recruit additional eyelid for surgical repair (Figure 2). The lateral eyelid was held with digital tension to expose the temporal aspect of the conjunctiva. A horizontal 2 mm transconjunctival incision was made using electrocautery approximately 3 mm superior to the tarsus, just lateral to the lateral canthal tendon. A Jaeger lid plate was placed adjacent to the conjunctival incision, and the electrocautery device was used to strum and identify the superior crux of the lateral canthal tendon. These attachments were severed using the electrocautery unit. The lateral eyelid could then be reapproximated.
The tarsus was closed with two lamellar 5-0 absorbable braided polyglactin 910 sutures. The orbicularis was closed with a single 5-0 polyglactin 910 suture. A small amount of redundant cutaneous tissue was excised using a Burrow’s triangle along the relaxed skin tension lines inferolaterally. The eyelid margin was repaired with a vertical mattress 7-0 silk suture, which was then run superiorly to close the skin. The silk suture was removed 2 weeks after surgery. Antibiotic ointment was placed on the surgical wounds. | |
|
Figure 2
A, Large upper eyelid coloboma B, Edges of the defect are freshened with #15 blade and an initial attempt at direct approximation failed to close the defect. C, The conjunctiva is incised approximately 3 mm superior to the tarsus in the right upper eyelid lateral fornix, and the superior crux of the lateral canthal tendon is lysed with a monopolar cautery instrument. D, The wound edges are precisely anastomosed without undue tension.
 |
|
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in