Dalia V. Zhang, BS | Cleveland Clinic Cole Eye Institute, Cleveland, Ohio Rao V. Chundury, MD, MBA | Glick Eye Institute, Indiana University, Indianapolis, Ohio Alexander D. Blandford, MD | Cleveland Clinic Cole Eye Institute, Cleveland, Ohio Julian D. Perry, MD | Cleveland Clinic Cole Eye Institute, Cleveland, Ohio
Eyelid colobomas are rare congenital malformations caused by failure of the mesodermal lid folds to fuse during embryogenesis. The resultant defect is often triangular in shape and located at the junction of the medial and middle 1/3 of the upper eyelid, although the shape, size, and location are all highly variable.(1) Colobomas are most commonly idiopathic and can present at birth as an isolated finding, but they may also be accompanied by systemic features, as in Goldenhar or Fraser syndrome.(7) Given the constellation of our patient’s signs and symptoms a presumptive diagnosis of Goldenhar syndrome was made.
Correction of large upper eyelid defects in the neonatal period presents unique challenges, because unilateral lid-sharing procedures can result in significant amblyopia. When possible, surgery may be delayed until the age of 3 or 4 years, when more lid tissue is available and the risk of induced amblyopia is decreased.(3) However, especially in larger defects, as in this case, surgery should be performed promptly to lessen or prevent exposure keratopathy. Historically, sliding tarsoconjunctival/myocutaneous flaps,(4) skin grafts,(5) or large lateral myocutaneous flaps(3) have been used with varying success.
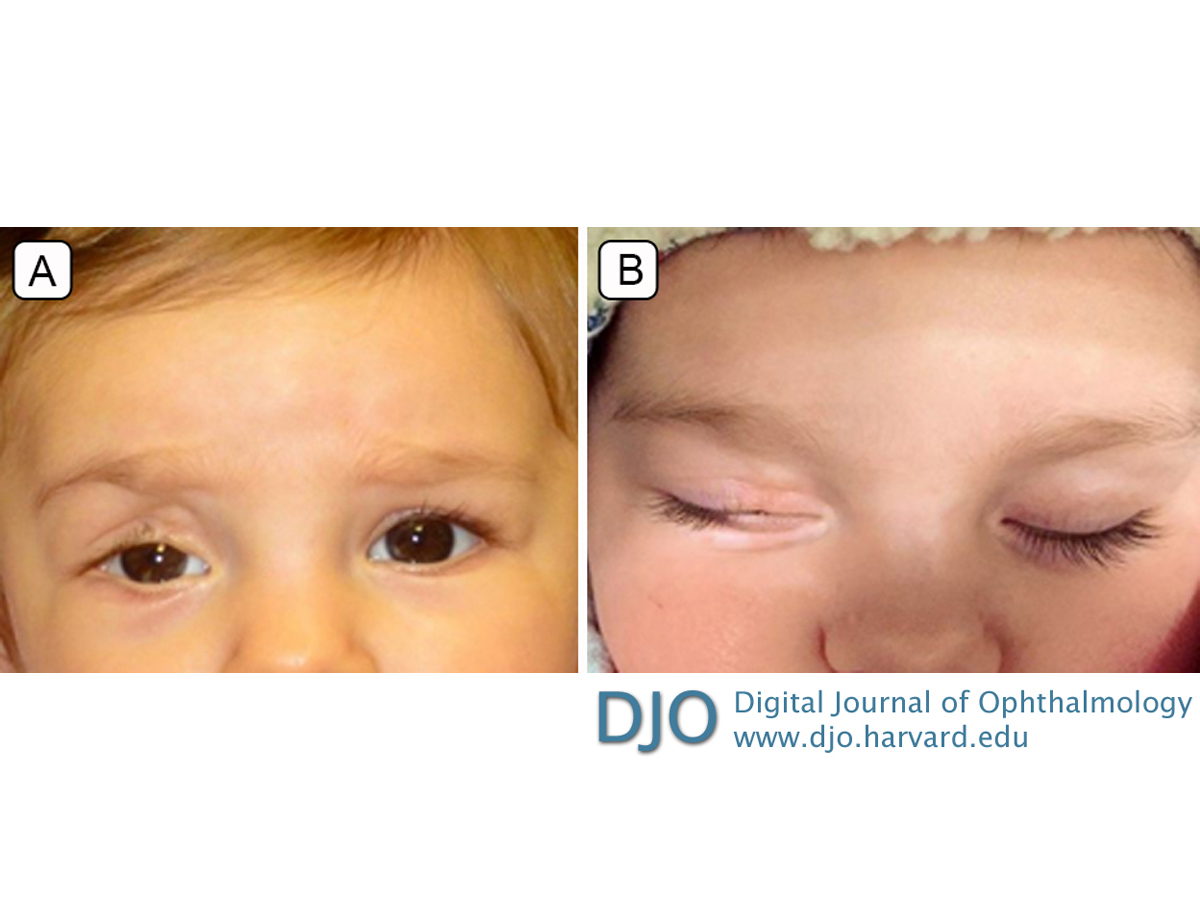
In this case, we used internal cantholysis followed by direct closure to repair the large right upper eyelid coloboma. The silk sutures were removed 3 weeks after surgery. A video taken at this time demonstrates excellent eyelid movement and contour (Video 1). At 9 months’ follow-up, there was a favorable eyelid contour, mild ptosis that did not obstruct the visual axis, and very slight lagophthalmos, without noticeable notch formation (Figure 3). There was persistence of superomedial periorbital hollowing, because the severe coloboma also involved the super superomedial fatty tissues in addition to the full thickness of the eyelid. Artificial tear ointment and drops were no longer necessary.
This technique produced significant lid mobility and avoided complications associated with other procedures commonly used for closure of large wounds, such as external scar formation and prolonged occlusion of vision. Although we did not encounter lateral canthal dystopia or lid buckling in this patient, such complications tend to be temporary and improve spontaneously in the early postoperative period.6 In the event that the amount of recruited tissue is initially inadequate, the procedure can easily be converted intraoperatively into a semicircular flap to allow for wound closure. The technique requires minimal equipment, requires no supplementary sutures, and produces excellent cosmetic and functional results, which is especially important in cases with potential for good visual outcome. Internal cantholysis is easily learned and is a powerful technique that should be considered as an option for repairing larger full-thickness lid defects in both adults and children.
 Welcome, please sign in
Welcome, please sign in