|
|
 |
|
|
|
|
|
29 year old woman with loss of visual field in her right eye
Digital Journal of Ophthalmology 1999
Volume 5, Number 8
January 8, 1999
|
Printer Friendly
|
|
|
|
|
|
|
| Diagnosis and Discussion | Post-partum Branch Retinal Artery Obstruction
The diagnosis was branch retinal artery obstruction due to protein S and protein C deficiency, presumably induced by pregnancy.
Retinal artery obstruction is rare in young patients. The associated etiologic factors are often diverse and different FROM those underlying artery obstruction in an elderly patient. Patients commonly have various factors leading to hypercoagulable state or embolic conditions. Cardiac valvular disease, history of migraine, hypercoagulable state due to pregnancy, Oral Contraceptive Pill usage, obesity, omocystinuria and hyperhomocytienemia are some of the documented associations. A hypercoagulable state can also be induced by protein S and protein C deficiency and Anti-phospholipid syndromes. Protein C and protein S are vitamin-k dependent anticoagulants. Activated protein C inhibits the clotting cascade by inhibiting factor V and factor VIII. Protein S acts as co-factor in activation of protein C. The deficiency of either factor can be inherited or acquired. An Inherited deficiency is transmitted as an autosomal dominant trait. The deficiency can be acquired in conditions like septic shock, disseminated intravascular coagulation, acute respiratory distress syndrome, post-operative states, liver diseases, pregnancy, Oral Contraceptive Pill use, patients with human immuno-deficiency virus infection and chemotherapy for breast cancer.
The prevalence of inherited protein C and protein S deficiency is 5% to 8% in young individuals with thrombotic events. In 60% to 70% of the patients with inherited Protein C or Protein S deficiency, thrombotic events occur spontaneously, while the rest have some associated risk factors. Homozygous congenital deficiency can result in paediatric venous thrombosis and severe neo-natal purpura.
Deficiencies have been associated with branch retinal vein occlusion, central as well as branch retinal artery occlusion, amaurosis fugax and bilateral disc oedema secondary to dural sinus thrombosis. The protein levels are measured by variety of immunologic and functional techniques. Protein C, protein S, Anti-thrombin III and activated protein C resistance should be included in the laboratory evaluation of young patient with suspected thrombotic event. The last test was not carried out in our patient the plasma level of protein S was definitely suggestive of deficiency, likely to be transient deficiency induced by pregnancy. Indeed the levels returned to normal on repeat testing 8 weeks later. The protein C levels could have been at the lower end of the normal spectrum.
Anti-coagulants and thrombolytic agents are recommended to treat these deficiencies. On detection of pregnancy, the patient with inherited deficiency may be started on heparin. Anabolic steroids such as Danazolol and Stanazolol increase the levels of protein C but do not prevent thrombosis. Anabolic steroids have no role to play in treatment of protein S deficient patient. The patients with acquired transient deficiency can be treated either with oral anti-coagulants or low dose dispersible Aspirin, depending on the severity of the deficiency.
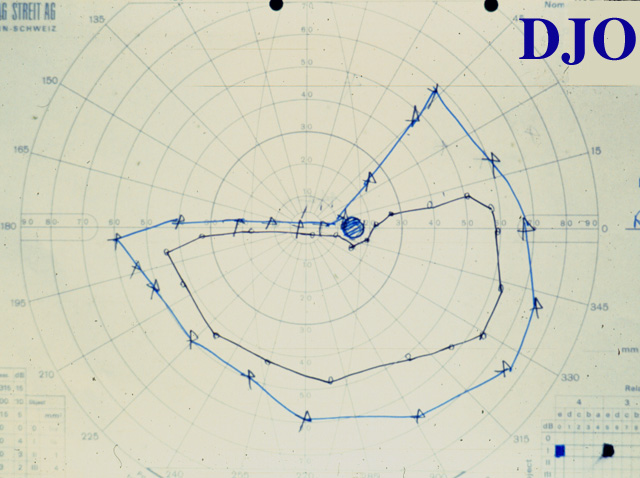
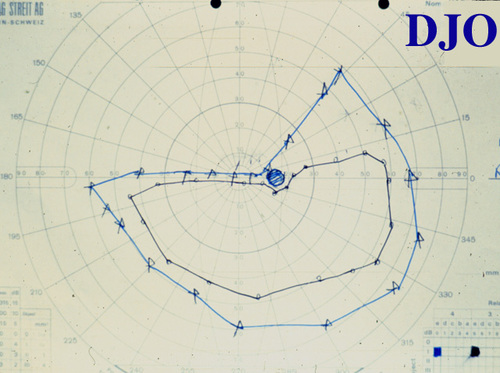
Our patient was treated with low dose Aspirin. Improvement in the visual field was noted on follow-up appointment 8 weeks later.(Figure 3) | |
|
Figure 3
Goldmanns' Visual Field testing demonstrating some recovery of visual field loss in the right eye 8 weeks later
 |
|
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in