|
|
 |
|
|
|
|
|
A 50-year-old man with a long-standing, large-angle exotropia and limitation of adduction in the left eye
Digital Journal of Ophthalmology 2013
Volume 19, Number 4
December 30, 2013
DOI: 10.5693/djo.03.2013.09.004
|
Printer Friendly
Download PDF |
|
|

Reshma A. Mehendale, MD | Department of Ophthalmology, Boston Children’s Hospital, and Harvard Medical School, Boston, Massachusetts Anat O. Stemmer-Rachamimov, MD | Department of Pathology, Massachusetts General Hospital, and Ophthalmic Pathology, Massachusetts Eye and Ear Infirmary, and Harvard Medical School Linda R. Dagi, MD | Department of Ophthalmology, Boston Children’s Hospital, and Harvard Medical School, Boston, Massachusetts
|
|
|
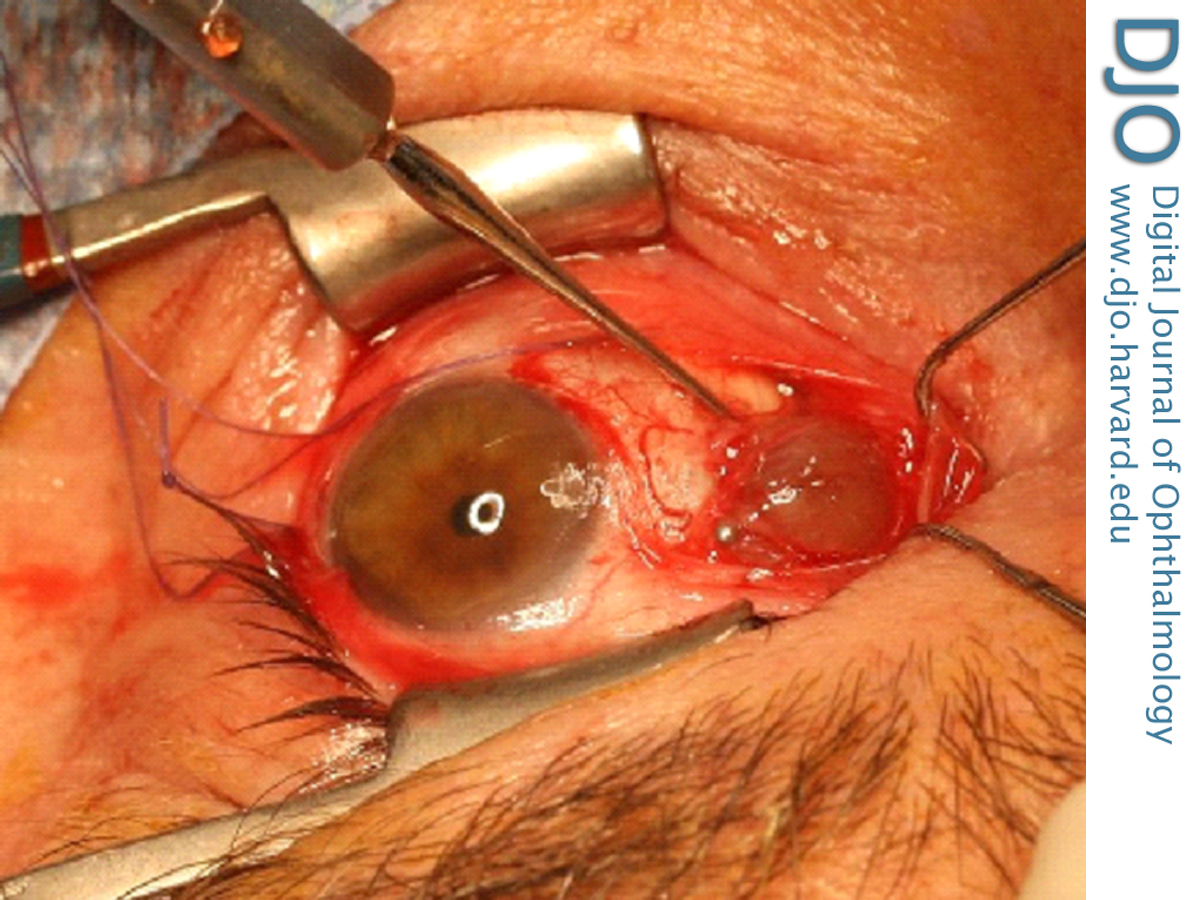
| Treatment | | Planned strabismus repair targeted the recovery and advancement of the “apparently slipped” medial rectus muscle, recession of the lateral rectus muscle and excision of the mass in toto, if possible. Intraoperative unroofing of a superficial layer of conjunctiva over the mass revealed a chocolate-colored cyst filled with sero-sanguninous fluid, with strands of flaccid extraocular muscle or pseudo-tendon straddling its surface (Figure 3). The color of the fluid was attributed to prior hemorrhage. Although excision in one piece proved technically challenging, an excisional biopsy of one large section of the mass included up to 10 mm of the flaccid medial rectus fibers. A gentle hand-over-hand technique was required to reach the posterior extension of the cyst, enabling recovery of the medial rectus muscle, well posterior to the equator and still attached to the posterior surface of the remaining wall of the cyst via a thin thread of muscle fiber. The body of the medial rectus muscle was recovered, advanced, and reattached to the anatomical insertion with an adjustable-suture technique after all visible remaining tissue from the cyst was surgically excised. The lateral rectus muscle was recessed on an adjustable suture. In the recovery room, the muscles were adjusted to a resultant esotropia of <10 PD at distance and at near. Mild limitation of adduction remained. Three months later, the patient’s sensorimotor examination demonstrated an exotropia of 8 PD at distance and 8-10 PD at near, with −1 limitation of adduction and −1.5 limitation of abduction. There has been no recurrence of the mass over a one-year follow-up period, and alignment has been stable. | |
|
Figure 3
Intraoperative appearance of the chocolate-colored cyst filled with serosanguninous fluid, with strands of flaccid extraocular muscle straddling its surface.
 |
|
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in