|
|
 |
|
|
|
|
|
A 31-year-old man with vitritis, chorioretinitis, and hydrocephalus
Digital Journal of Ophthalmology 2012
Volume 18, Number 2
May 14, 2012
DOI: 10.5693/djo.03.2012.03.001
|
Printer Friendly
Download PDF |
|
|
|
|
|
|
| Examination | On ophthalmic examination, visual acuity was 20/200 in the right eye, with pinhole improvement to 20/100, and 20/40 in the left eye, with pinhole improvement to 20/20. Ishihara color vision testing showed correct identification of 3 of 8 plates in the right eye and 8 of 8 plates in the left eye. There was a relative afferent pupillary defect present in the right eye. Slit-lamp examination revealed trace conjunctival injection in the right eye, along with small keratic precipitates on the inferior corneal endothelium and 3+ cell in the anterior chamber. The anterior segment of the left eye was normal. Normal and symmetric intraocular pressures were obtained.
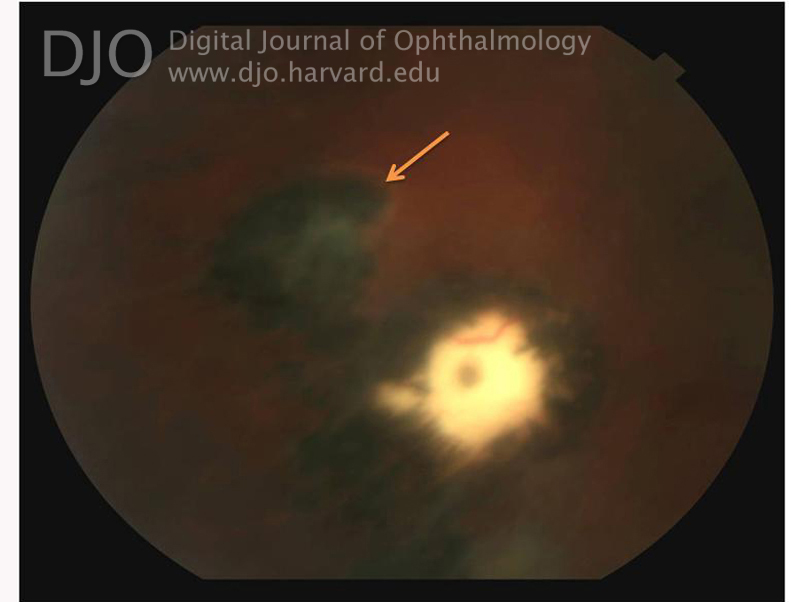
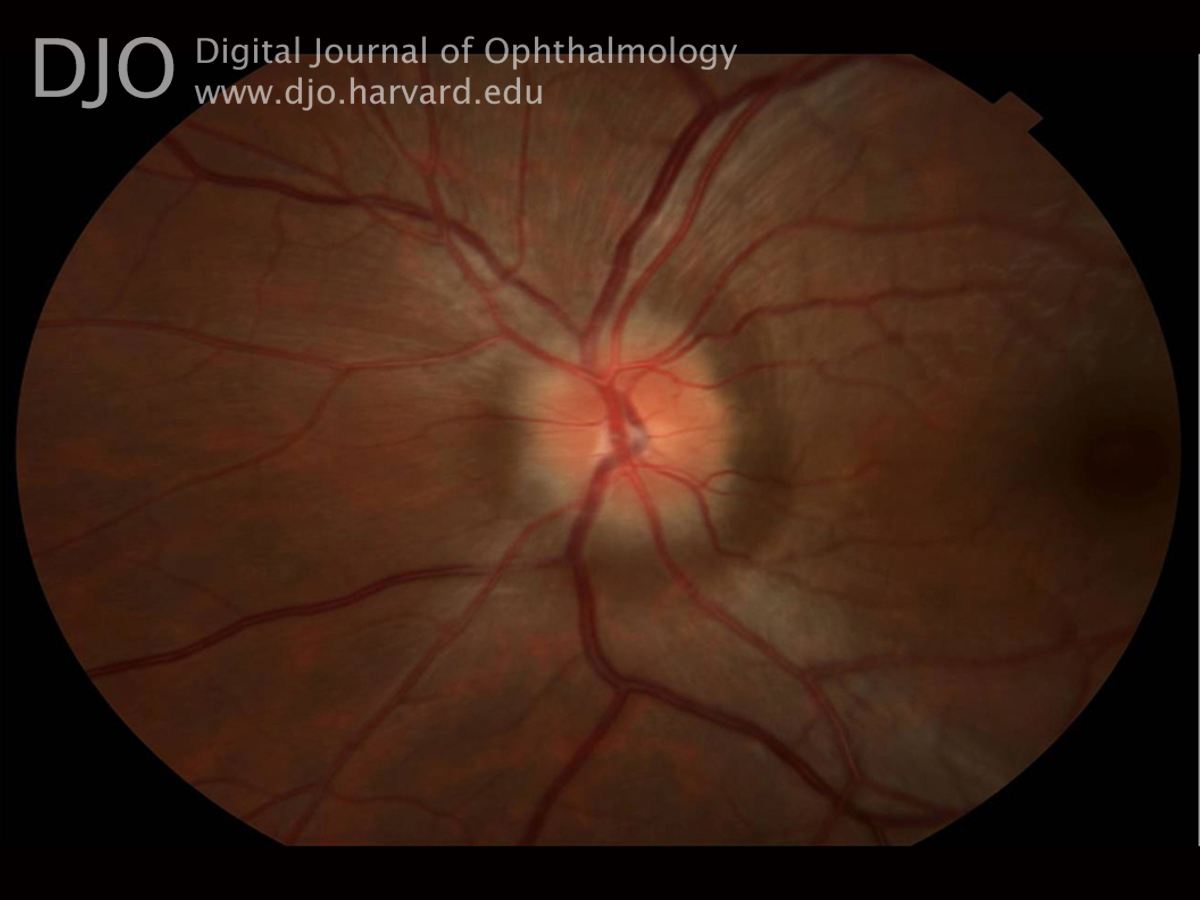
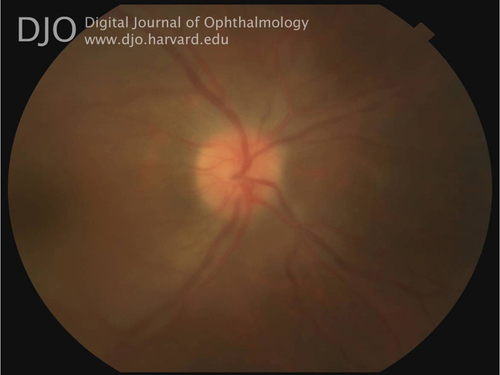
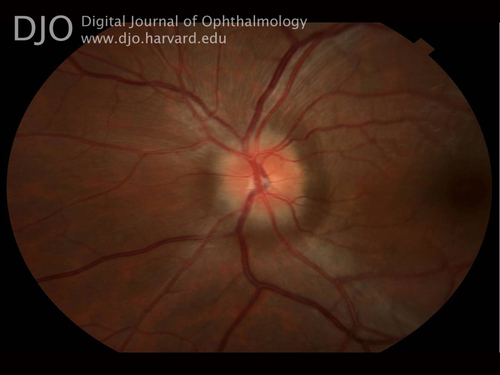
Dilated stereoscopic fundus examination revealed 2+ vitreous cell in the right eye and bilateral optic nerve head edema (Figures 1-2). Indirect ophthalmoscopy of the right eye demonstrated a large, pigmented, inferotemporal chorioretinal scar with a superjacent area of presumed retinitis (Figure 3). The macula and peripheral retina of the left eye were normal. | |
|
Figure 1
Right fundus, optic nerve head margins appear blurred. Details obscured due to vitritis.
 |
|
|
Figure 2
Right fundus, centered on chorioretinal lesion inferotemporal to macula. The lesion is notable for encircling pigment and the suggestion of retinitis at superior border (denoted by arrow).
 |
|
|
Figure 3
Left fundus showing optic disc edema.
 |
|
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in