|
|
 |
|
|
|
|
|
A 31-year-old man with vitritis, chorioretinitis, and hydrocephalus
Digital Journal of Ophthalmology 2012
Volume 18, Number 2
May 14, 2012
DOI: 10.5693/djo.03.2012.03.001
|
Printer Friendly
Download PDF |
|
|
|
|
|
|
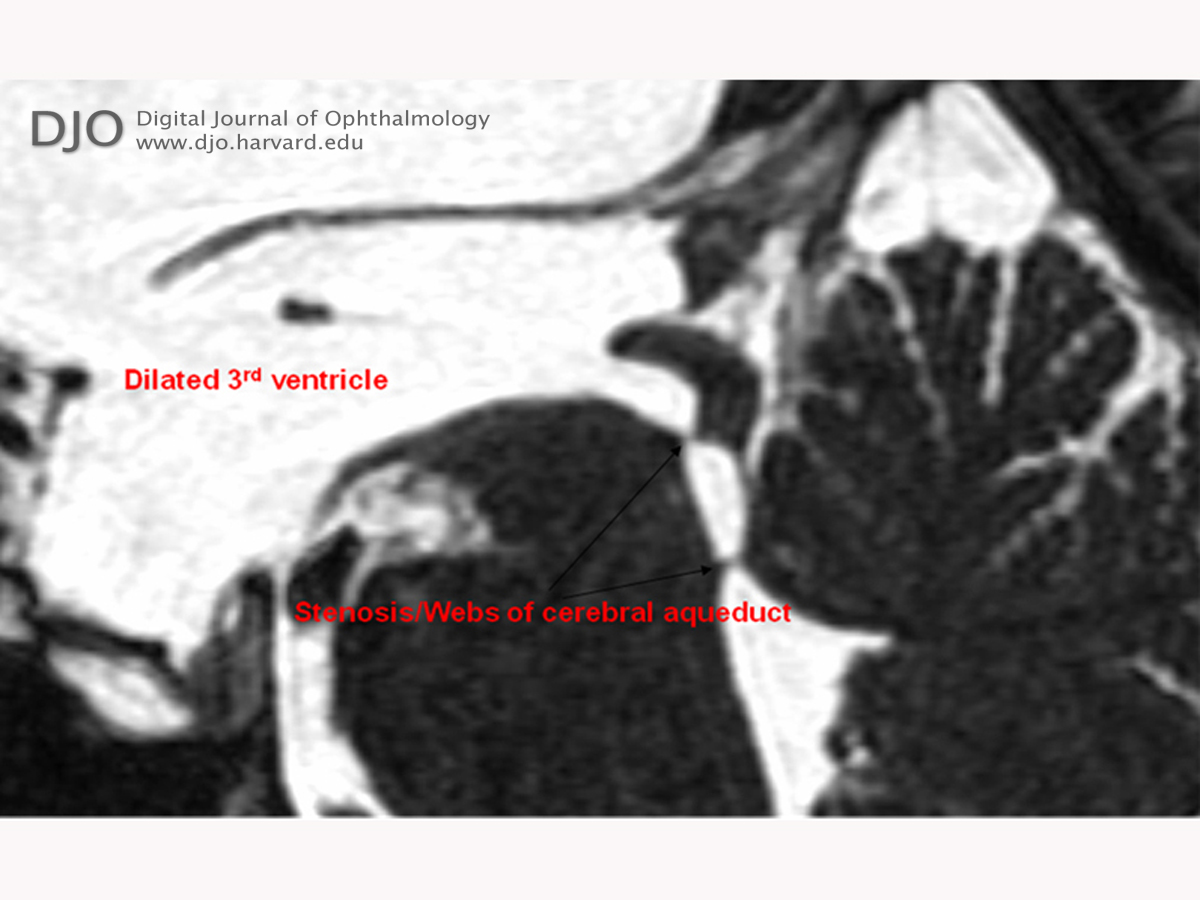
| Ancillary Testing | | The patient’s headache and disc edema warranted a referral to Massachusetts General Hospital for neuroimaging and evaluation. Our recommendations included serologic testing for HIV and toxoplasmosis. Computed tomography was performed without contrast and disclosed severe hydrocephalus likely related to cerebral aqueductal stenosis (Figure 4). An MRI scan with and without gadolinium contrast was ordered to further delineate the pathology; this revealed hydrocephalus with dilatation of the lateral and third ventricles with a normal-appearing fourth ventricle (Figures 5-6). The sagittal FIESTA protocol showed webs within the cerebral aqueduct and a lack of CSF flow through to the fourth ventricle. | |
|
Figure 5
MRI, T2 FIESTA protocol, sagittal view, delineating anatomy of ventricles and CSF flow.
 |
|
|
Figure 6
MRI FIESTA, coronal view, revealing engorgement of the lateral and 3rd ventricles.
 |
|
|
Figure 4
CT brain without contrast, axial view, revealing symmetric enlargement of the lateral ventricles.
 |
|
|
|
|
|
|
|
 Welcome, please sign in
Welcome, please sign in