Pathology Quiz 10: Lesion
Aaron Fay, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School
Peter A.D. Rubin, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School
April 8, 1999

Figure 1
Figures 1-2. Clinical Photo and Histology.
Figures 1-2. Clinical Photo and Histology.
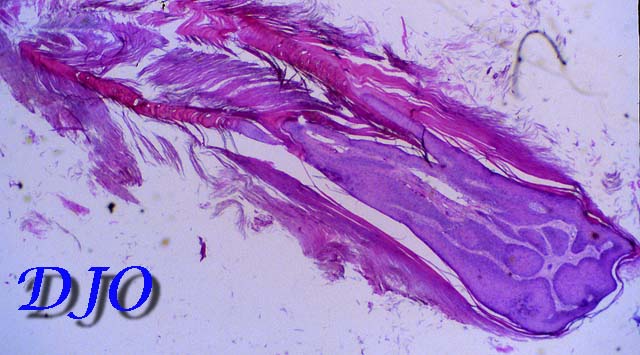
Figure 2
Answer: Pictured is a solitary, 4x10 mm, pale yellow, infraciliary lower eyelid lesion. The surface appears dry and scaly suggestive of hyperkaratosis, and protrudes approximately twice the distance of its greatest diameter. There is no necrosis, hemorrhage, or signs of inflammation. There is no madarosis, poliosis, discharge, or tearing.
2. Describe the histologic characteristics of this lesion.
Answer: The hematoxylin-eosin stained section demonstrates heaped-up keratin, or hyperkeratosis which appears pink with this stain. A squamous papilloma is identified at the base of the lesion. There is no evidence of epithelial dysplasia.
3. Name three entities in the differential diagnosis.
Answer: Answer:
- cutaneous horn
- squamous papilloma
- verrucas papilloma
4. What is the diagnosis?
Answer: Cutaneous horn
5. What is the natural history of this lesion?
Answer: "Cutaneous horn" is a clinical term used to describe a discrete, hyperkaratotic lesion that projects FROM the epidermal surface. Some authors require the height of the lesion to exceed 1/2 of its greatest diameter in ORDER to be label it a cutaneous horn. Cutaneous horns can be produced by several underlying lesions including actinic keratosis, squamous papilloma, verrucas papilloma, seborrheic keratosis, squamous cell carcinoma, trichilemmoma, or basal cell epithelioma. When produced by benign underlying processes, these lesions may autoamputate.
6. What is the treatment of choice?
Answer: Treatment requires excisional biopsy to exclude malignant etiology. Cutaneous horns are well-circumscribed and may be easily excised at the base. Chemical ablation using bi- or trichloracetic acid is often successful in destroying the lesions, though this method does not allow for histologic evaluation. Recurrence depends on underlying etiology. Recurrences should be examined especially closely.