Pathology Quiz 8: Lesion
Aaron Fay, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School
Peter A.D. Rubin, MD | Massachusetts Eye and Ear Infirmary, Harvard Medical School
February 8, 1999

Figure 1
Figures 1-2. Clinical Photo and Histology.
Figures 1-2. Clinical Photo and Histology.
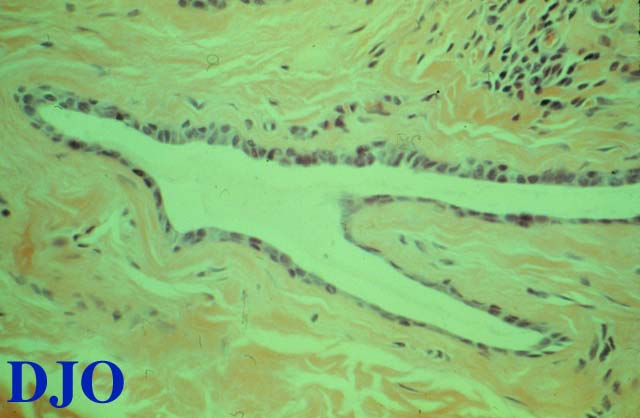
Figure 2
Answer: The clinical photograph demonstrates multiple round, skin-colored, elevated eyelid lesions involving the upper and lower eyelids, ranging in size FROM 1 to 8 mm, located anterior to the lash line without lid margin involvement. The larger lesions appear cystic. The surface is smooth without evidence of umbilication, ulceration, or hyperkaratosis. There is no hemorrhage, trichiasis, discharge, or associated conjunctivitis.
2. Describe the histologic characteristics of this lesion.
Answer: The hematoxylin-eosin stained section demonstrates a bilayered epithelium-lined cyst located within a connective tissue stroma. There is evidence of mild adjacent chronic, non-granulomatous inflammation (lymphocytes without epithelioid cells). There are no dermal adnexal structures seen in this section. No apical snouting is seen, and no material is seen within the cyst cavity.
3. Name three entities in the differential diagnosis.
Answer: Answer:
- Moll's gland cysts
- hidrocystoma
- sudoriferous cysts
- ductal cysts
- epithelial inclusion cysts
- basal cell carcinoma (inferomedial)
- molluscum contagiosum
4. What is the diagnosis?
Answer: Answer:
- hidrocystoma
- sudoriferous cyst
- ductal cyst
5. What is the natural history of this lesion?
Answer: The nomenclature for eyelid cysts is somewhat confusing owing to the multitude of glandular elements within the eyelid. "Hidrocystoma," "sudoriferous ("sweat") cyst," and "ductal cyst" are synonymous terms used to describe cystic sweat gland lesions. Most sweat glands throughout the human body of are the eccrine variety; they secrete directly INTO the glandular lumen via exocytosis. Some areas of the body, including the axilla, groin, ear canal, and eyelids, include apocrine sweat glands; they secrete INTO the glandular lumen by pinching off the apical portions of the cells surrounding the lumen (apical snouting). In the eyelid, apocrine hidrocystomas arise FROM the glands of Moll. Hidrocystomas are distinguished FROM other eyelid cysts by the presence of a bilayered epithelial lining. The inner cuboidal layer secretes INTO the lumen; the outer layer is composed of myoepithelial cells. Hidrocystomas are benign lesions that may cause chronic irritation. They are seen with equal frequency among men and women. There is no race predilection. Individuals prone to systemic hidrosis and those chronically exposed to warm moisture may be at increased risk.
6. What is the treatment of choice?
Answer: Treatment usually requires excision with complete removal of the cyst wall, though chemical destruction can be accomplished using bi- or trichloracetic acid. Spontaneous resolution is not usually seen. Mechanical rupture as sometimes performed at home by patients may result in infection and rarely provides permanent collapse of the cysts.