Neuro-ophthalmology Quiz 4
Howard Pomeranz, M.D., Ph.D. | Massachusetts Eye and Ear Infirmary, Harvard Medical School, University of Maryland Medical Center
M.A. Afshari, M.D., M.P.H. | Massachusetts Eye and Ear Infirmary, Harvard Medical School
August 1, 1997

Figure 1
Figures 1-2. Fundus
Figures 1-2. Fundus
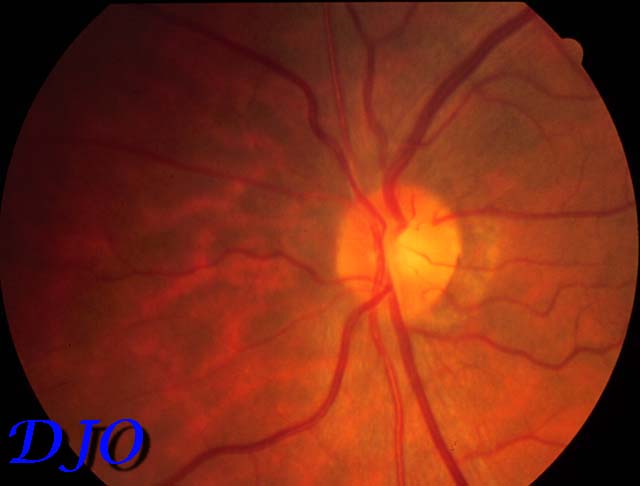
Figure 2
Answer: Optic nerve sheath meningioma. This tumor arises FROM the arachnoid lining of the optic nerve and slowly enlarges. It is a benign tumor which eventually surrounds and strangles the optic nerve causing blindness. The tumor may occur at any age but most people are 30 to 50 years of age at diagnosis and 75% of patients are female. Patients with this tumor may have disk edema without evidence of optic nerve dysfunction. With long-standing disk edema bright spots may develop in the disk substance. The diagnostic appearance of this tumor on a CT scan is the so-called "tram track" sign in the optic nerve meninges in axial sections with calcification. Patients may develop optociliary collaterals (retinal to vortex vein collaterals) on the surface of the optic nerve head when optic atrophy occurs. Patients with optic nerve sheath meningioma may exhibit gaze-evoked amaurosis. Because the tumor encases the optic nerve patients can develop ischemic compression of the optic ! nerve with gaze in a particular direction. This tumor is benign and does not kill the patient. Excision is controversial but may be advised the patients under the age of 20 to prevent intracranial extension of the tumor. Most patients are observed and tend to do poorly in the affected eye. Radiation treatment may be considered but may result in radiation optic neuropathy. The illustration in this case shows optociliary shunt vessels on the surface of the optic nerve.