A 77 year old man with diplopia
Digital Journal of Ophthalmology 2004
Volume 10, Number 11
November 19, 2004
Volume 10, Number 11
November 19, 2004
Past Medical History: None
Past Ocular History: Bilateral cataract extractions (OS 5 months prior to OD) by clear corneal incision phacoemulsification procedures performed under inferior peribulbar anaesthetic using a mixture of 2% lignocaine and 0.5% bupivacaine administered by an experienced anaesthetist.
Current Medications: None
Pupillary examination - Normal OU
Ocular Motility -
Primary position: 40 prism diopter (PD) right hypotropia and 8 PD right exotropia.
Right gaze: 35 PD right hypotropia.
Left gaze: 30 PD right hypotropia.
Up and right gaze: 35 PD right hypotropia.
Down and right gaze: 35 PD right hypotropia.
Up and left gaze: 30 PD right hypotropia.
Down and left gaze: 30 PD right hypotropia.
Forced duction testing revealed a marked restriction of elevation of the right eye.
Tonometry: Normal OU
Slit lamp examination of the anterior segment: Normal OU
Fundus examination: Normal OU without torsion.
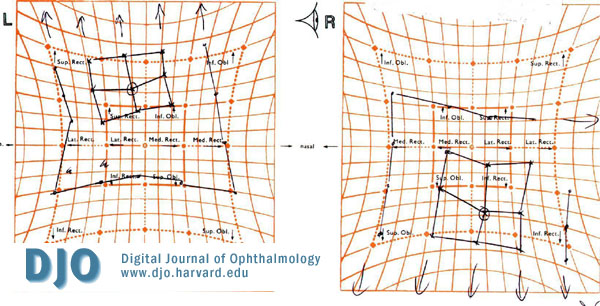
Figure 1
Hess chart 7 months after cataract extraction demonstrating marked vertical muscle imbalance.
Hess chart 7 months after cataract extraction demonstrating marked vertical muscle imbalance.

Figure 2
Motility examination
Motility examination
Chest X-ray – Normal
Computed tomography scanning of the orbits was performed and revealed an isolated segmental enlargement of the inferior rectus muscle in the right eye.
Pathology
TSH: Normal
Thyroid antibodies - Normal
Erythrocyte sedimentation rate – Normal
C-reactive protein (CRP) - Normal
Full blood count – Normal
Anti-Neutrophilic Cytoplasmic Antibodies (ANCA) – Normal

Figure 3a
CT scan demonstrating normal size inferior rectus
CT scan demonstrating normal size inferior rectus
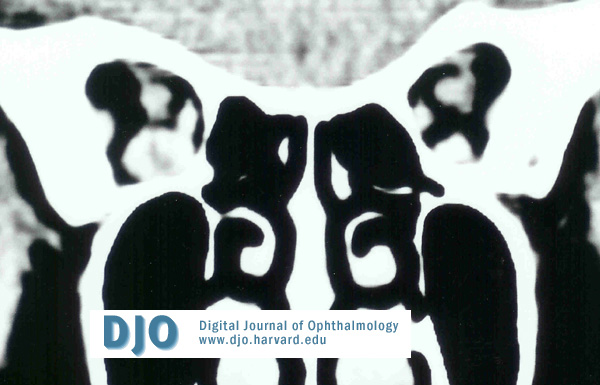
Figure 3b
Enlarged inferior rectus in the posterior orbit
Enlarged inferior rectus in the posterior orbit
· Orbital pseudotumour – myositis
· Wegener’s granulomatosis
· Orbital metastatic disease
· Ocular muscle fibrosis following anaesthetic trauma
Persistent binocular diplopia is a rare complication of cataract extraction and is estimated to occur in 0.2 to 0.3% of cases [1,2]. The diplopia is thought to be the result of trauma to one or more extra-ocular muscles, either directly through needle trauma or bridle sutures or indirectly through the myotoxic effect of local anaesthetic [3-6]. The myotoxicity of local anaesthetics (lignocaine, mepivacaine and bupivacaine) have been clearly illustrated in experimental studies on rats, primates and humans [7,8]. In all cases the histological findings supported destruction of virtually all muscle fibres in the infiltrated muscles. Carlson et al found minimal muscle regeneration in the human study and suggests the patients advanced age as a contributory factor for increased fibrosis. The inferior rectus muscle was affected in up to 80% of all cases [2, 9-12]. Muscle injury can cause paresis, over action or contracture. Contracture or fibrosis follows an initial period of paresis but, as this case demonstrates, patients do not present during the paretic phase, as they only become symptomatic weeks or months after the surgery. It has been suggested that left eyes are more commonly involved as right-handed professionals who may have difficulty with access to the left eye give most of the anaesthetic blocks [2,13]. MR or CT imaging techniques has shown segmental thickening or enlargement of the inferior rectus muscle in patients with restriction following cataract extraction [9,14].
There is consensus in the literature regarding the treatment of these cases with the vast majority of authors suggesting recession of the restricted muscle using an adjustable suture technique if the diplopia cannot be controlled with prisms. The results appear to be extremely good with most patients achieving fusion after surgery with or without prisms.
A sub-tenon’s or topical local anaesthetic technique has been suggested to reduce the risk of this complication although there have been case reports implicating sub-tenon’s anaesthesia in strabismus following cataract extraction [15,16].
In conclusion, diplopia following cataract extraction is a rare complication but all patients should be told about the possibility of postoperative diplopia and strabismus. The vast majority of cataract surgery is performed in an elderly population, which may reduce the chances of regeneration of the affected muscle with an increase in subsequent fibrosis and contracture.
2. Pearce IA, et al. Vertical diplopia following local anaesthetic cataract surgery: predominantly a left eye problem? Eye 2000; 14(2): 180-184
3. Catalano RA, et al. Persistent strabismus presenting after cataract surgery. Ophthalmology 1987; 94:491
4. Burns, C.L. and Seigel, L.A.: Inferior rectus recession for vertical diplopia after cataract surgery, Ophthalmology 1988; 95:1120
5. Freeman, R.S.: Diplopia following cataract surgery Am. Orthopt. J.1994; 44:2
6. Wylie, J. et al: persistent binocular diplopia following cataract surgery: Etiology and management, Eye 1994; 8:543
7. Carlson BM, Rainin EA. Rat extra-ocular muscle regeneration: repair of local anaesthetic induced damage. Arch Ophthalmol 1985; 103:1373-7
8. Carlson BM, et al. Extraocular muscle regeneration in primate: Local anaesthetic-induced lesions. Ophthalmology1992; 99:582-9
9. Hamed, LM, Mancuso A. Inferior rectus muscle contracture syndrome after retrobulbar anaesthesia, Ophthalmology1991; 98:1506-12
10. de Faber JT, von Noorden GK. Inferior rectus muscle palsy after retrobulbar anaesthesia for cataract surgery. Am J Ophthalmol 1991; 112:209-11
11. Hamed, L.M.: Strabismus presenting after cataract surgery, Ophthalmology 1991;98:247-52
12. Capo H, Roth E, et al. Vertical strabismus after cataract surgery. Ophthalmology 1996; 103:918-21
13. Corboy JM, Jiang X. Postanaesthetic hypotropia: a unique syndrome in left eyes. J Cataract Surg 1997; 23:1394-8
14. Hamilton SM, Elsas FJ, Dawson TL. A cluster of patients with inferior rectus restriction following local anaesthesia for cataract surgery. J Pediatr Ophthalmol Strabismus 1993; 30:288-91
15. Jaycock PD, Mather CM, Ferris JD, et al. Rectus muscle trauma complicating sub-tenon’s local anaesthesia. Eye 2001; 15(5): 583-6
16. Spierer A, Schwalb E. Superior oblique muscle paresis after sub-tenon’s anaesthesia for cataract surgery. J Cat Refract Surg 1999; 25(1): 144-5