47 year old man with a peripheral retinal lesion found on routine exam
Digital Journal of Ophthalmology 1997
Volume 3, Number 23
July 30, 1997
Volume 3, Number 23
July 30, 1997
Michael A. Kapusta, M.D., FRCS(C) | Doheny Eye Institute, University of Southern California, Los Angeles, California
Michael B. Yang, M.D. | Doheny Eye Institute, University of Southern California, Los Angeles, California
Talia Kolin, M.D. | Doheny Eye Institute, University of Southern California, Los Angeles, California
Lawrence P. Chong, M.D. | Doheny Eye Institute, University of Southern California, Los Angeles, California
PMHx: none
Meds: none
SHx: Non contributory
FHx: Non contributory
Pupils: Equal, reactive, No APD
Amsler grid: no metamorphopsia OU
Visual Field: full to confrontation
Motility: Full OU
Applanation pressure: normal OU
Slit lamp examination: normal anterior segments OU
Fundus examination: See Figures 1-2
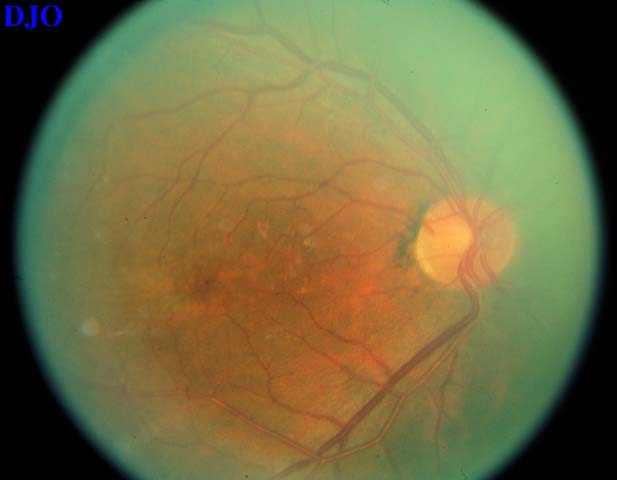
Figure 1a
Figures 1a-1b. There is mild mottling of the retinal pigment epithelium in the macula OU
Figures 1a-1b. There is mild mottling of the retinal pigment epithelium in the macula OU

Figure 1b
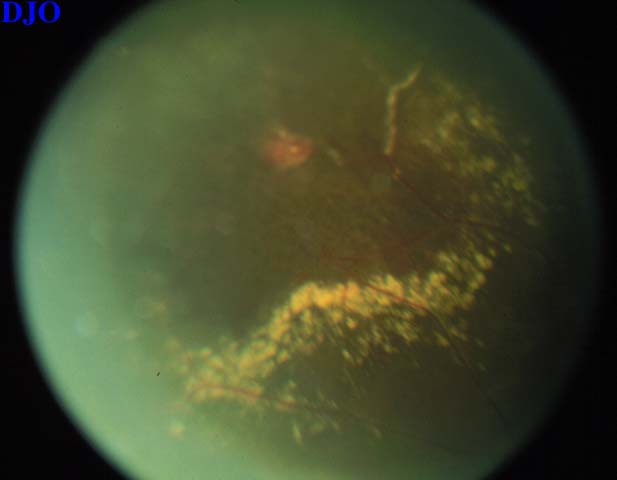
Figure 2
In the right eye, there is a peripheral area of hyperpigmentation supratemporally with an adjacent area of exudative change surrounding an aneurysm.
In the right eye, there is a peripheral area of hyperpigmentation supratemporally with an adjacent area of exudative change surrounding an aneurysm.
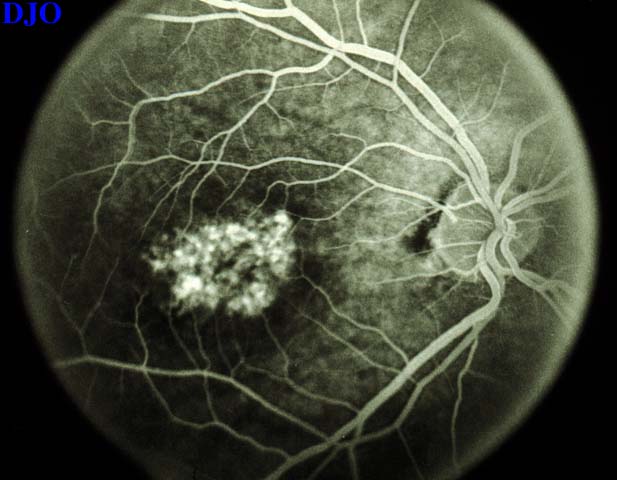
Figure 3a
Figures 3a-3b. Fluorescein angiogram showed punctate areas of hyperfluorescence in the parafoveal region of both eyes. This hyperfluorescence was consistent with window defects due to abnormalities in the region of the macula.
Figures 3a-3b. Fluorescein angiogram showed punctate areas of hyperfluorescence in the parafoveal region of both eyes. This hyperfluorescence was consistent with window defects due to abnormalities in the region of the macula.
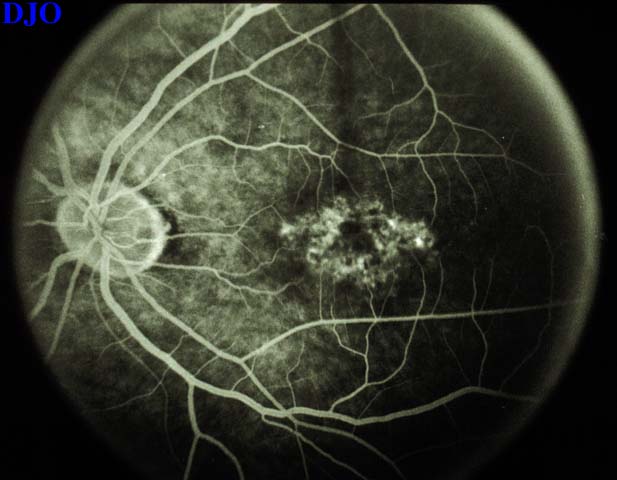
Figure 3b
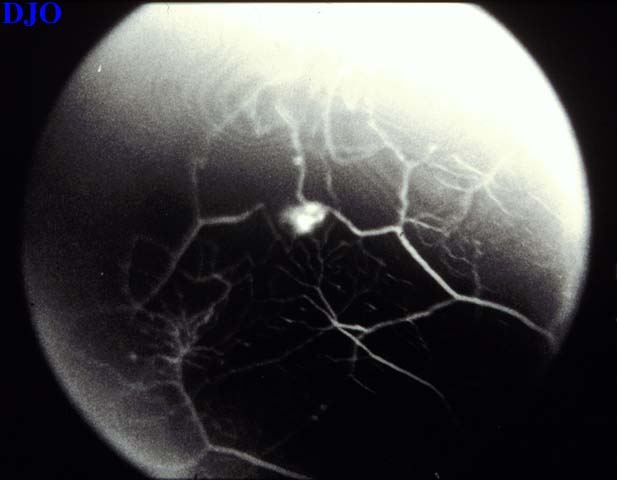
Figure 4a
Figures 4a-4c. Supratemporally, in the peripheral retina of the right eye, there was an exudative process surrounding an aneurysm. In this area, the angiogram demonstrated capillary nonperfusion as well as saccular and beadlike dilatations of the retinal vessels. Dilatation of the surrounding capillary bed was also seen. The aneurysm showed early staining and late leakage. The aneurysm had no prominent feeder or drainage vessels.
Figures 4a-4c. Supratemporally, in the peripheral retina of the right eye, there was an exudative process surrounding an aneurysm. In this area, the angiogram demonstrated capillary nonperfusion as well as saccular and beadlike dilatations of the retinal vessels. Dilatation of the surrounding capillary bed was also seen. The aneurysm showed early staining and late leakage. The aneurysm had no prominent feeder or drainage vessels.
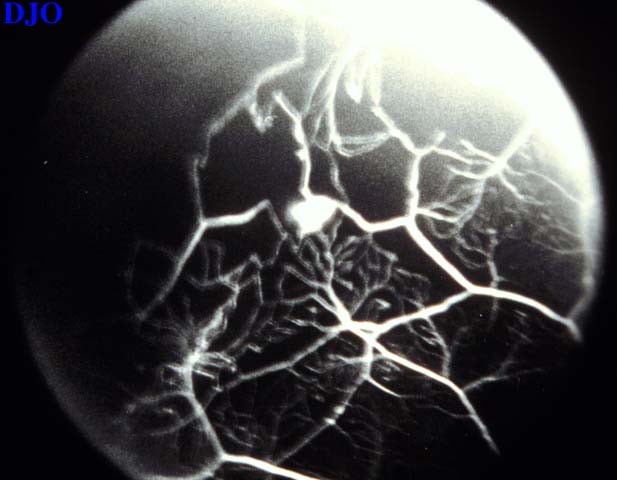
Figure 4b
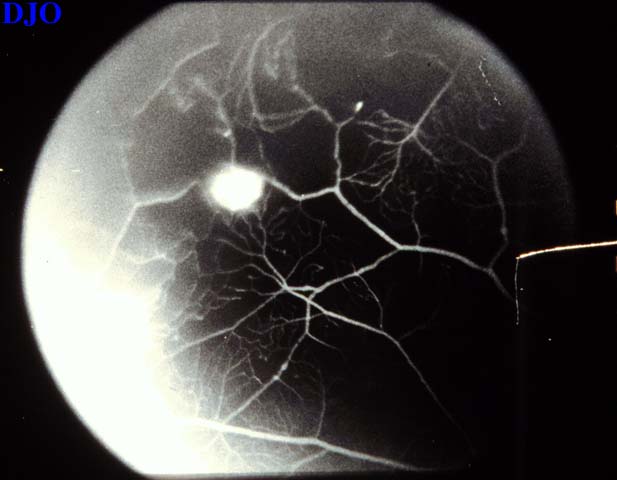
Figure 4c
- Macroaneurysm
- Retinal Angioma
Coats' disease is characterized by massive hard exudates associated with congenital retinal telangiectasias. Vascular anomalies including fusiform venous dilatation, microaneurysms, perivasculitis, collateral vessels, and nonperfusion of the retina, may be present in variable degrees. Hemorrhage may occur, as well. Abnormal vessels leak INTO and under the retina. Exudation tracking under the retina is termed as a Wise response. When such exudation is accompanied by a sensory retinal detachment, it is termed as a Coats' response. This may appear, clinically, as leukocoria. While initially painless, Coats' disease may progress to glaucoma, retinal detachment, cataract, and phthisis.
Coats' disease occurs in males three to eight times more frequently than females. There is no inheritance pattern or racial predilection. It is unilateral in 80% of cases. The common adolescent form occurs before the age of sixteen. It tends to progress faster in children under the age of four. Less frequently, patients present at a later age with the adult form.
Our patient presented at age 27 with a vascular anomaly that was diagnosed as Coats' disease. There was no family history. The previous lesion was unilateral and treated extensively with laser photocoagulation. The new lesion was found adjacent to the area of photocoagulation and was characterized by exudates and retinal thickening surrounding an area of capillary nonperfusion with vessel dilatation. The aneurysm in the center of this area did not have a feeding or draining vessel, which would be characteristic of a retinal angioma. Therefore, further investigations of the brain and kidneys for the presence of aneurysms was deemed unnecessary. Ultrasonography and fine-needle aspiration biopsy may be helpful in differentiating advanced Coats' disease FROM other causes of leukocoria, especially in cases where it is necessary to rule out malignancy. Our patient presented at an early stage, with a benign process. Echography and biopsy were not indicated.
The patient was treated with photocoagulation to the aneurysmal lesion to stimulate its closure. Grid photocoagulation to the surrounding retina was also performed to promote resolution of retinal edema.
2) Stewart J, Halliwell T, Gupta RK. Cytodiagnosis of Coats' disease FROM an ocular aspirate. A case report. Acta Cytologica 37(5): 717-720, 1993
3) Patel HK, Augsburger JJ, Eagle RC. Unusual presentation of advanced Coats' disease. J Pediatr Ophthalmol Strab 32(2): 120-122, 1995
4) Senft SH, Hidayat AA, Cavender JC. Atypical presentation of Coats' disease. Retina 14(1):36-38, 1994
5) Coats' Disease. Julia A. Haller. Retina . Stephen J. Ryan Editor in Chief. Mosby. Medical Retina Volume 2. Second edition Chapter 84. Page 1453-1460, 1994
6) Atta HR, Watson NJ. Echographic diagnosis of advanced Coats' disease. Eye 6(1): 80-85, 1992
7) Smirniotopoulos JG , Bargallo N, Mafee MF: Differential diagnosis of leukokoria: radiologic-pathologic correlation. Radiographics 14(5): 1059-1079, 1994
8) Kubota T, Kurihara K, Ishibashi T, Inomata H. Proliferative vitreoretinopathy in Coats' disease. Clinicopathological case report. Ophthalmologica 209(1):44-46, 1995
9) Schmidt, EU,Lucke K. Vitreoretinal surgery in advanced Coats' disease. Ger J Ophthalmol 4(1):32-36, 1995
10) Yoshizumi MO, Krieger AE, Lewis H.et al. Vitrectomy techniques in late-stage Coats'-like exudative retinal detachment. Documenta Ophthalmol 90(4): 387-394, 1995