Bilateral uveal effusions in a 23-year-old man
Digital Journal of Ophthalmology 2018
Volume 24, Number 2
May 22, 2018
DOI: 10.5693/djo.03.2018.03.001
Volume 24, Number 2
May 22, 2018
DOI: 10.5693/djo.03.2018.03.001
Karen W. Jeng-Miller, MD, MPH | Department of Ophthalmology, Massachusetts Eye and Ear Infirmary, Harvard Medical School, Boston, Massachusetts
Eric D. Gaier, MD, PhD | Department of Ophthalmology, Massachusetts Eye and Ear Infirmary, Harvard Medical School, Boston, Massachusetts
Angela V. Turalba, MD | Department of Ophthalmology, Atrius Health, Boston, Massachusetts
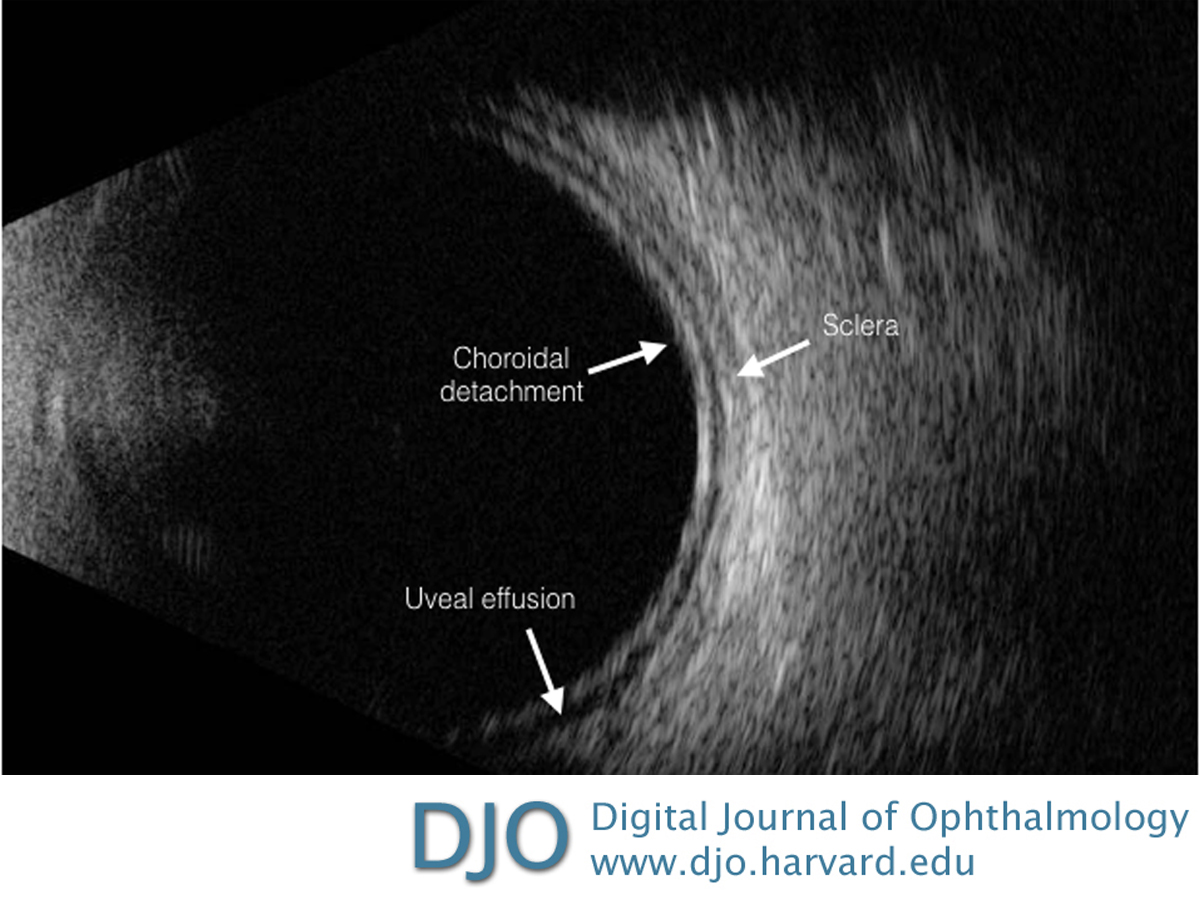
Figure 1
B-scan ultrasound of the left eye showing uveal effusion and no evidence of an intraocular mass. The same findings were present in the right eye.
B-scan ultrasound of the left eye showing uveal effusion and no evidence of an intraocular mass. The same findings were present in the right eye.
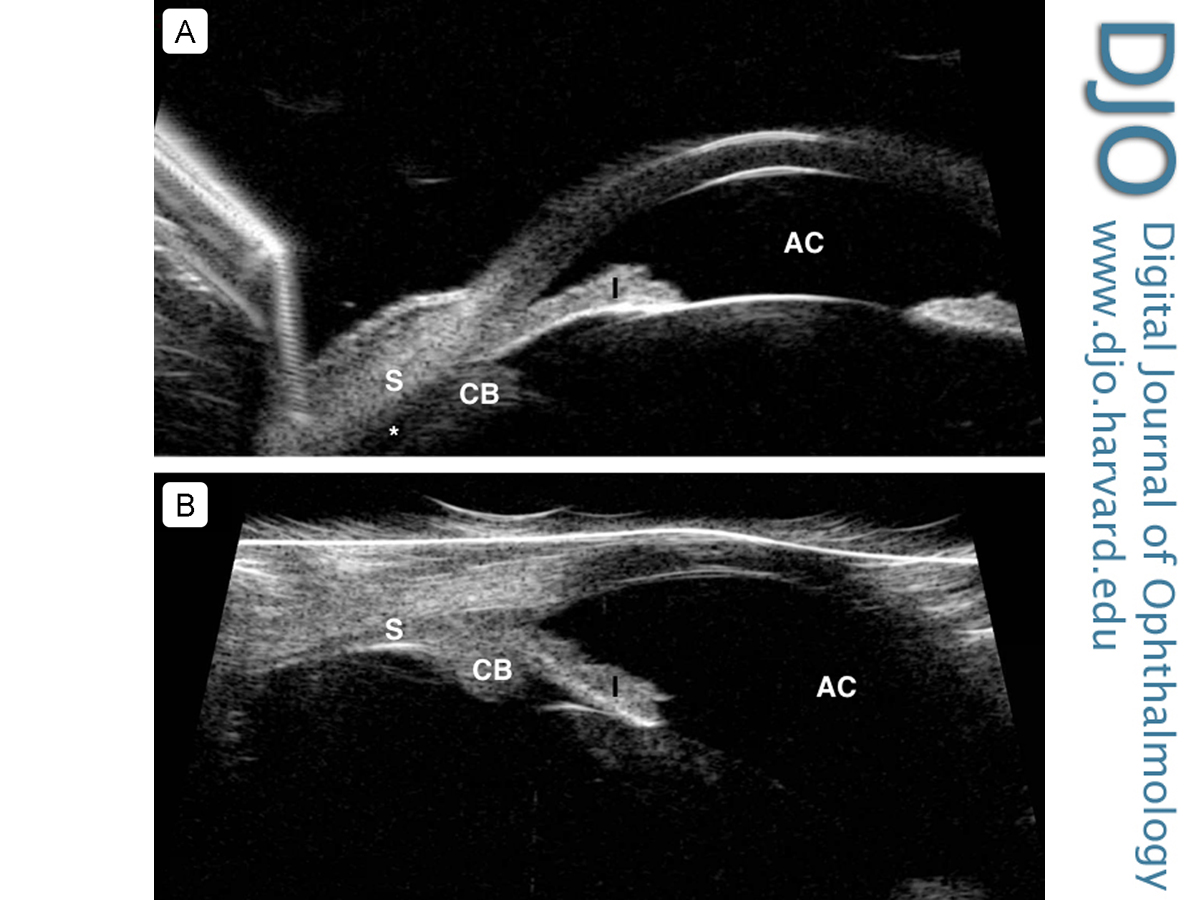
Figure 2
A, Ultrasound biomicroscopy (UBM) of the left eye showing evidence of peripheral uveal effusion (asterisk) and shallow anterior chamber (AC). The same findings were present in the right eye. B, UBM of the left eye demonstrating resolution of the peripheral uveal effusions with deepening of the anterior chamber. CB, ciliary body; I, iris; S, sclera.
A, Ultrasound biomicroscopy (UBM) of the left eye showing evidence of peripheral uveal effusion (asterisk) and shallow anterior chamber (AC). The same findings were present in the right eye. B, UBM of the left eye demonstrating resolution of the peripheral uveal effusions with deepening of the anterior chamber. CB, ciliary body; I, iris; S, sclera.
Also as part of the assessment, a thorough dilated fundus examination is essential, with particular attention to assessing for vitritis and retinal/choroidal masses. Our patient had no masses or vitritis on examination, supporting our suspicion of a pharmacological or idiopathic etiology. Biometry measurements did not reveal a nanophthalmic eye. The patient did endorse taking a single dose of a new muscle relaxant provided by a friend 10 days earlier, although the specific drug was unknown, and the patient was unable to find this information. The timeline in this case is consistent with a drug-induced uveal effusion. A postviral etiology for the bilateral uveal effusions was initially considered. Mansour et al reported unilateral uveal effusion following H1N1 influenza infection;(16) however, the patient cited an episode of diarrhea only 1 day prior to his symptoms, making this etiology less likely.
Our report is unfortunately limited by the unknown type and dose of medication consumed by our patient, which was reportedly a muscle relaxant. Furthermore, he did not undergo a manifest refraction to objectively document the myopic shift as a result of the uveal effusions; nor did he receive a urine toxicology screen to definitely rule out other agents resulting in his presentation.
Once the diagnosis of pharmacologic-induced uveal effusion syndrome is established, treatment usually consists of medication cessation, topical cycloplegic agents to lower IOP via posterior rotation of ciliary process, and topical/oral antihypertensive drops. In these cases, the mechanism of secondary angle closure is not via pupillary block; therefore, a peripheral iridotomy is ineffective relieving the angle closure. However, argon laser peripheral iridoplasty has been successfully used as initial therapy.(8)
Literature Search
PubMed was searched without restriction on November 28, 2017, using the following terms: bilateral uveal effusion and muscle relaxant uveal effusion.
2. Chan KCY, Sachdev N, Wells AP. Bilateral acute angle closure secondary to uveal effusions associated with flucloxacillin and carbamazepine. Br J Ophthalmol 2008;92:428-30.
3. Fraunfelder FW, Fraunfelder FT, Keates EU. Topiramate-associated acute, bilateral, secondary angle-closure glaucoma. Ophthalmology 2004;111:109-11.
4. de Guzman MHP, Thiagalingam S, Ong PY, Goldberg I. Bilateral acute angle closure caused by supraciliary effusions associated with venlafaxine intake. Med J Aust 2005;182:121-3.
5. Postel EA, Assalian A, Epstein DL. Drug-induced transient myopia and angle-closure glaucoma associated with supraciliary choroidal effusion. Am J Ophthalmol 1996;122:110-2.
6. Reis GM, Lau OC, Samarawickrama C, Heydon P, Goldberg I. Utility of ultrasound biomicroscopy in the diagnosis of topiramate-associated ciliochoroidal effusions causing bilateral acute angle closure. Clin Experiment Ophthalmol 2014;42:500-1.
7. Roh Y-R, Woo SJ, Park KH. Acute-onset bilateral myopia and ciliochoroidal effusion induced by hydrochlorothiazide. Korean J Ophthalmol 2011;25:214-7.
8. Sbeity Z, Gvozdyuk N, Amde W, et al. Argon laser peripheral iridoplasty for topiramate-induced bilateral acute angle closure. J Glaucoma 2009;18:269-71.
9. Singer JR, Pearce ZD, Westhouse SJ, Siebert KJ. Uveal effusion as a mechanism of bilateral angle-closure glaucoma induced by chlorthalidone. J Glaucoma 2015;24:84-6.
10. Takusagawa HL, Hunter RS, Jue A, Pasquale LR, Chen TC. Bilateral uveal effusion and angle-closure glaucoma associated with bupropion use. Arch Ophthalmol 2012;130:120-2.
11. Végh M, Hári-Kovács A, Réz K, Tapasztó B, Szabó A, Facskó A. Indapamide-induced transient myopia with supraciliary effusion: case report. BMC Ophthalmol 2013;13:58.
12. Zelefsky JR, Fine HF, Rubinstein VJ, Hsu IS, Finger PT. Escitalopram-induced uveal effusions and bilateral angle closure glaucoma. Am J Ophthalmol 2006;141:1144-7.
13. Murphy RM, Bakir B, O’Brien C, Wiggs JL, Pasquale LR. Drug-induced bilateral secondary angle-closure glaucoma: a literature synthesis. J Glaucoma 2016;25:e99-105.
14. Sharif NA, Senchyna M. Serotonin receptor subtype mRNA expression in human ocular tissues, determined by RT-PCR. Mol Vis 2006;12:1040-7.
15. Martin XD, Brennan MC, Lichter PR. Serotonin in human aqueous humor. Ophthalmology 1988;95:1221-6.
16. Mansour DEAA, El-Shazly AA-F, Elawamry AI, Ismail AT. Comparison of ocular findings in patients with H1N1 influenza infection versus patients receiving influenza vaccine during a pandemic. Ophthalmic Res 2012;48:134-8.