44 year old man with incidental orbital mass
Digital Journal of Ophthalmology 2002
Volume 8, Number 2
February 1, 2002
Volume 8, Number 2
February 1, 2002
Peter A.D. Rubin, M.D.,F.A.C.S. | Massachusetts Eye and Ear Infirmary, Harvard Medical School, Boston, MA
Gabriel Garza M.D. | Massachusetts Eye and Ear Infirmary, Harvard Medical School, Boston, MA
Mark P. Hatton, M.D. | Massachusetts Eye and Ear Infirmary, Harvard Medical School, Boston, MA
Past Ocular History: none
Past Medical History: Sinusitis
Medications: None
Family History: Non-contributory.
Pupils: Equal, round, and reactive to light. No afferent pupillary defect
Color vision: Normal OU
Motility: Full OU
Exophthalmometry: 5 mm proptosis of the left globe.
Slit lamp exam: normal OU
Fundus exam: normal OU
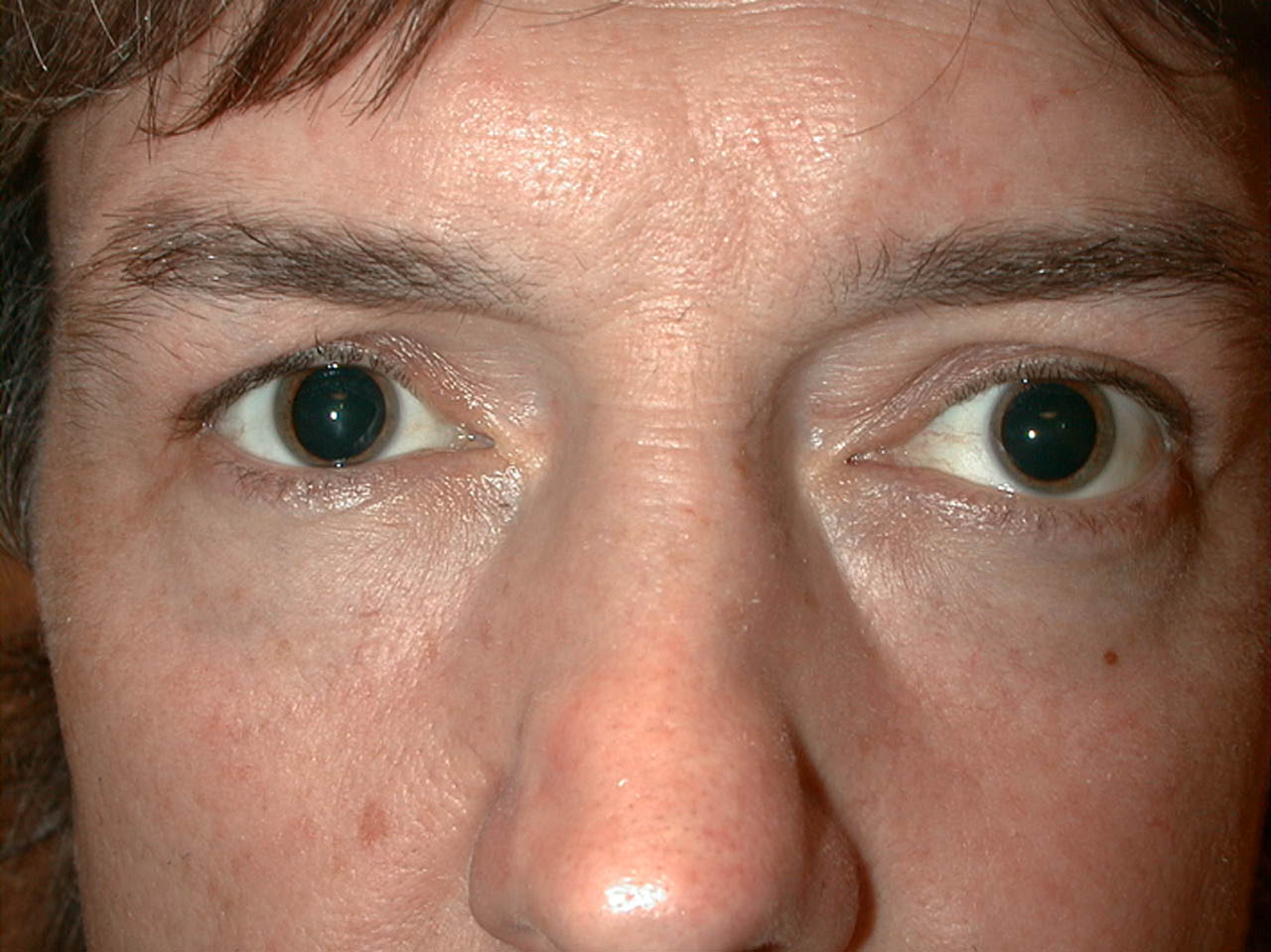
Figure 1a

Figure 1b
Pathology
The results of special stains were:
CD34: positive
Vimentin: positive
S-100: negative
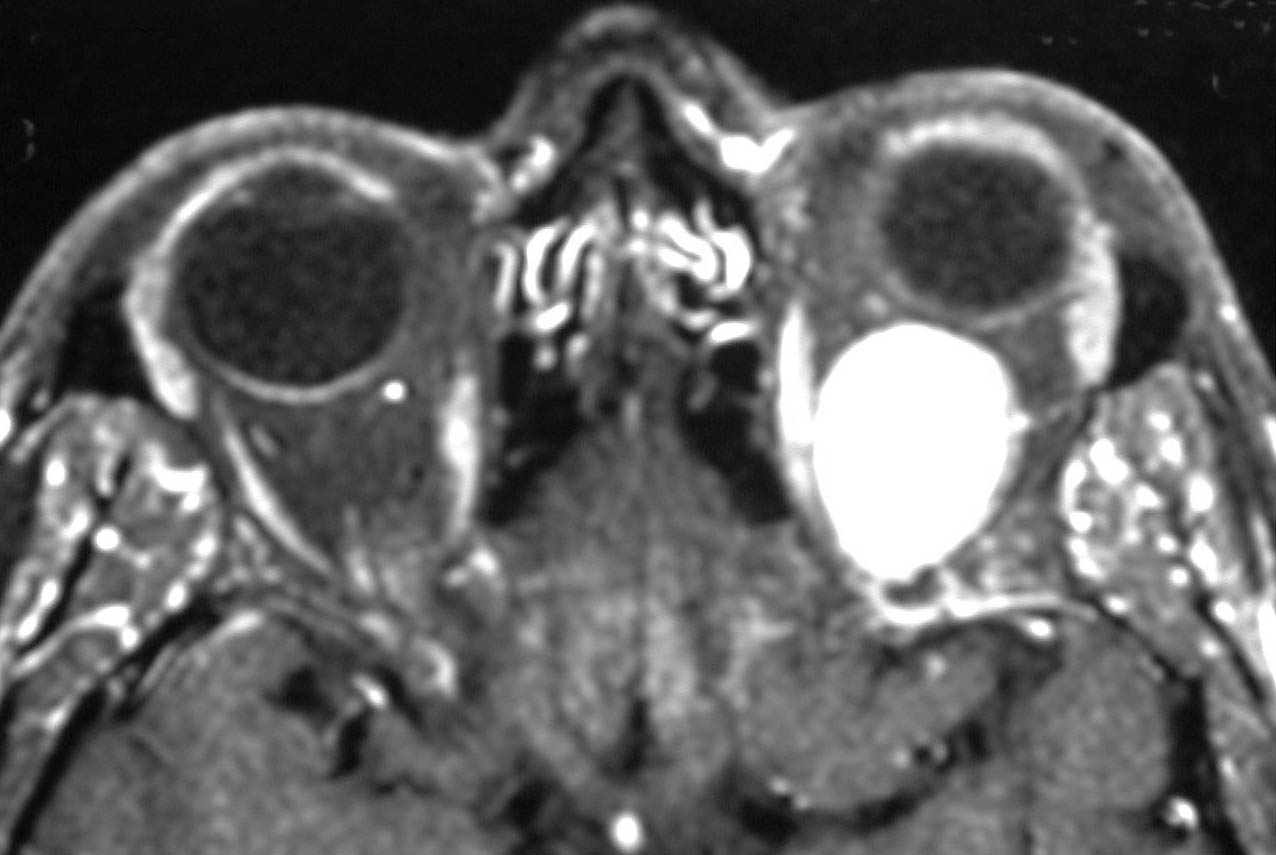
Figure 2
The CT scan reveals a well circumcscribed mass in the posterior, superior aspect of the left orbit.
The CT scan reveals a well circumcscribed mass in the posterior, superior aspect of the left orbit.
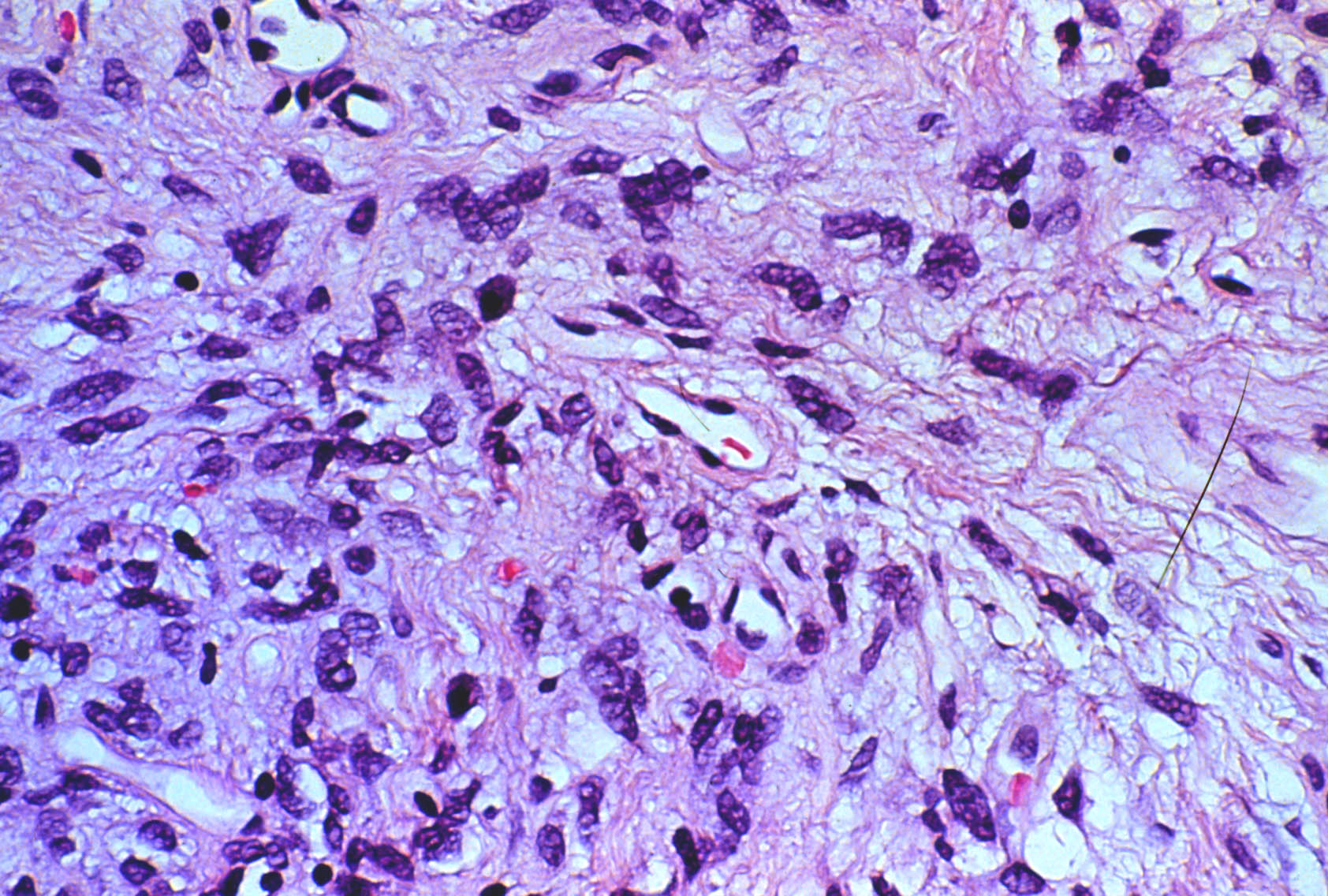
Figure 3
H&E staining demonstrates uniform collagen-forming spindle cells with minimal mitotic activity. Some cells SHOW myxoid changes. Vascularity is represented by narrow vascular clefts.
H&E staining demonstrates uniform collagen-forming spindle cells with minimal mitotic activity. Some cells SHOW myxoid changes. Vascularity is represented by narrow vascular clefts.
- Neurilemmoma
- Neurofibroma
- Cavernous hemangioma
- Hemangiopericytoma
- Lymphoma
- Metastasis
- Meningioma
- Fibrous tumor
Solitary fibrous tumors were first described in 1931. They were originally termed mesothelioma based on the assumption that they arose FROM mesothelial tissues, such as pleura, where they were first observed. Subsequently, they have been assigned various names in the literature, including localized fibrous mesothelioma, solitary fibrous mesothelioma, subserosal fibroma, and pleural fibroma (1). It is now accepted that the tumor arises not FROM mesothelium, but FROM mesenchyme (2). It has been renamed solitary fibrous tumor and has been reported in sites throughout the body.
Solitary fibrous tumors characteristically are well-circumscribed . Histology reveals alternating areas of hypo- and hyper-cellularity. Typically, the cells are spindle shaped, SHOW few mitotic figures, and appear to grow haphazardly in what has been called a "patternless pattern"(3). Cells which comprise the solitary fibrous tumor stain with markers for CD34 and vimentin, but not with cytokeratin or S-100 (4).
The first report of solitary fibrous tumor of the orbit appeared in 1994. To our knowledge, there have been 11 cases reported of orbital solitary fibrous tumor (5). They typically present with progressive, painless proptosis. Literature review suggests that 10-20% of solitary fibrous tumors throughout the body are malignant. To date, there have been no reported cases of metastases FROM orbital solitary fibrous tumors, although there has been one reported case of local recurrence following excision.
Fibrous tumors of the orbit are relatively rare. The most common fibrous tumor of the orbit is fibrous histiocytoma. Like solitary fibrous tumors, fibrous histiocytomas stain with vimentin. They are distinguished FROM solitary fibrous tumors based on their "storiform" growth pattern and their malignant potential (6). Distinguishing benign FROM malignant tumors radiographically is difficult, but may be aided by magnetic resonance imaging (7).
Current management of solitary fibrous tumors of the orbit is surgical resection with periodic follow-up to monitor for recurrence.
2. Dervan, P.A., Tobin, B., and O'Connor, M. Solitary (localized) fibrous mesothelioma: evidence against mesothelial cell origin. Histopathology. 1986; 10:867-75
3.Dorfman, D., To, K., Dickersin, G., Rosenberg, A., and Pilch, B. Solitary fibrous tumor of the orbit. American Journal of Surgical Pathology. 1994;18:281-7.
4 Westra, W., Gerald, W., and Rosai, J. Solitary fibrous tumor. Consistent CD34 immunoreactivity and occurrence in the orbit. American Journal of Surgical Pathology. 1994;18:992-8.
5. Ing, E.B., Kennerdell, J.S., Olson, P.R., Ogino, S., and Rothfus, W.E. Solitary fibrous tumor of the orbit. Ophthalmic Plastic and Reconstructive Surgery. 1998;14:55-67.
6. Rodrigues, M.M, Furiuele, F.P, and Weinreb, S. Malignant fibrous histiocytoma of the orbit. Archives of Ophthalmology 1987;95:2025-8.
7. Dalley, R.W. Fibrous histiocytoma and fibrous tissue tumors of the orbit. Radiology Clinics of North America 1999;37:185-94.