43 year old man with 3 days of blurry vision OS
Digital Journal of Ophthalmology 2002
Volume 8, Number 7
August 1, 2002
Volume 8, Number 7
August 1, 2002
Nisha Acharya, M.D. | Massachusetts Eye and Ear Infirmary
Previous ocular history: presbyopia
Past Medical History: none
Medications: none
Family and Social History: non-contributory
Pupils: Normal OU, no APD
Motility: Full OU
Tonometry: Normal OU
Slit Lamp Examination: Normal anterior segements
Fundus Examination: Normal OD; OS Figure 1
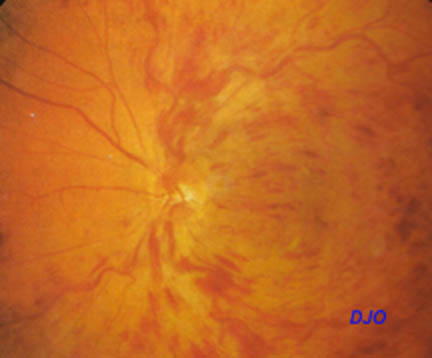
Figure 1
Diffuse intraretinal hemorrhage and dilated/tortuous retinal vasculature.
Diffuse intraretinal hemorrhage and dilated/tortuous retinal vasculature.
- Severe hypertensive retinopathy
- Radiation retinopathy
- Retinopathy of carotid artery occlusive disease
- Central retinal vein occlusion (CRVO)
Central retinal vein occlusions (CRVO) result FROM thrombosis at and posterior to the level of the lamina cribrosa. An atherosclerotic central retinal artery may impinge on the central retinal vein, causing turbulent flow, endothelial damage and thrombus formation. 90% of patients are older than 50 yrs of age at onset, and the male to female incidence is 3:2. CRVO may be bilateral in 6-14% of cases, and the risk of vascular occlusion in the fellow eye is 1% per year. Risk factors for CRVO include systemic hypertension, diabetes mellitus, open angle glaucoma, hyperviscosity syndromes, vasculitis, and hypercoagulability .
CRVOs may be categorized as non-ischemic or ischemic. Non-ischemic CRVOs have less than 10 disc areas of retinal capillary nonperfusion on angiogram. Anterior segment neovascularization is rare in these patients. Ischemic CRVOs (greater than 10 disc areas of retinal capillary nonperfusion) occur in approximately 30% of cases. They exhibit more extensive hemorrhage, retinal edema and venous dilation than non-ischemic CRVOs. Visual prognosis for ischemic CRVO patients is poor, with 10% of eyes achieving acuity better than 20/400. Up to 60% of patients with the ischemic variety will develop iris neovascularization (mean onset 3-5 months after onset of CRVO).
There is no proven benefit of aspirin, steroids, or systemic anticoagulation in the treatment of CRVO. Patients are monitored for the development of iris neovasculaization, and pan-retinal photocoagulation is performed if it develops. Underlying systemic conditions should be treated (hypertension/diabetes). Additionally, CRVO in young patients should prompt an evaluation for a hypercoaguable state.